





Abstract
Nonthrombotic pulmonary embolism (NTPE) is defined as embolisation to the pulmonary circulation of different cell types (adipocytes, haematopoietic, amniotic, trophoblastic or tumour), bacteria, fungi, foreign material or gas. The purpose of this article is to describe the clinical signs, pathogenesis, diagnosis and treatment of the different NTPE subtypes.
The complex and diverse pathogenesis of different subtypes of emboli is subject to continuing speculation and is certainly far more complex than “simple” mechanical obstruction after embolisation of vascular thrombi. Nonthrombotic emboli may also lead to a severe inflammatory reaction both in the systemic and pulmonary circulation, as well as in the lung.
NTPE presents a formidable diagnostic challenge, as the condition often presents with very unusual and peculiar clinical signs that are frequently overlooked. They range from very dramatic acute presentations such as acute respiratory distress syndrome to signs observed late in the disease course. Pathological observations play a key role in the exact diagnosis, and sometimes carefully aspirated blood from the pulmonary artery or specific staining of cells recovered from bronchoalveolar lavage fluid may be helpful. Frequently, lung biopsies revealing severe granulomatous reaction or unfortunate post-mortem pathological investigations of pulmonary tissue are necessary to confirm the diagnosis. Here, we also aim to familiarise the reader with the atypical radiological features of NTPE. Thin-section computed tomography of the lungs showing peculiar radiographic findings, such as a feeding vessel, the so-called tree-in-bud pattern or the appearance of micronodules distributed at the termination of bronchovascular bundles, may be observed in certain forms of NTPE.
Increased awareness of NTPE as an underestimated cause of acute and chronic embolism, which may result in acute and chronic pulmonary hypertension, is needed. Despite the fact that detailed descriptions of several forms of NTPE have existed for nearly 100 years, well-designed trials have never been performed to evaluate therapy in the different subsets of these patients.
Unlike pulmonary thromboembolism, a frequently encountered cause of morbidity and mortality 1, nonthrombotic pulmonary embolism (NTPE) is less common. NTPE often presents with uncharacteristic clinical features and requires peculiar diagnostic measures and treatment options. Different cell types (adipocyte, haematopoietic, amniotic, trophoblastic or tumour), bacteria, fungi, foreign material and gas may be carried in the bloodstream and embolise to the pulmonary circulation (fig. 1⇓). In contrast to “ordinary” thrombotic pulmonary embolism (PE), the effects of NTPE are not purely mechanical but are also linked to the nature of the embolic agent. This implies that the pathogenesis of NTPE is more complex than that of pulmonary thromboembolism and it is subject to continued speculation 2. Nevertheless, NTPE can be associated with specific imaging findings, and familiarity with these features should facilitate prompt diagnosis 3. This article reviews the features of acute and chronic NTPE.

Nonthrombotic pulmonary embolism (NTPE) is characterised as embolisation to the pulmonary circulation of different cell types (adipocytes, haematopoietic, amniotic, trophoblastic or tumour), bacteria, fungi, foreign material or gas. NTPE presents a diagnostic challenge, as the condition often presents with very unusual and peculiar clinical signs that are frequently overlooked. They range from very dramatic acute presentations, such as acute respiratory distress syndrome (ARDS) after fat and amniotic embolism, to signs observed late in the disease course, such as after tumour emboli. Moreover, paradoxical nonthrombotic emboli may cause cerebral signs and symptoms.
FAT EMBOLISM
As early as in 1861, fat droplets were described in the lung of a railway worker who had sustained a crush injury 4. Fat embolism (FE) is characterised by the release of fat into the systemic circulation. Fat embolism syndrome (FES) is a rare clinical consequence of FE, typified by the triad of pulmonary distress, mental status changes and a petechial rash 5.
Incidence
Disruption of sinusoids and fat in bone marrow allows fat globules and bone debris to gain access to the venous circulation. Embolisation of bone fat probably occurs in almost all patients who sustain a pelvic or long-bone fracture or undergo an endomedullary nailing of long-bone fractures or placement of knee and hip prosthesis 6. An autopsy study of soldiers who died in the Second World War revealed a 65% incidence of pulmonary fat droplets 7. 0.25–11% of patients who sustain a single long-bone fracture meet the criteria of FE 5, 8, 9. FES is more frequent in patients with multiple fractures 10, with an incidence of 4.8–7.5% after bilateral femoral fractures 11. FES is observed mostly after bone fractures of lower extremities, less frequently with upper extremity fractures, and rarely after rib fractures or vertebral injury 12.
FE is not limited to skeletal injury. It is the leading cause of respiratory deterioration in blast victims who survive 13. As no evidence of myeloid tissue was found in lung sections from blunt trauma victims, it is believed that soft tissue is the source of FE in these cases 14. The almost ubiquitous finding of FE in cases of natural death is attributed to resuscitative measures 15.
Other causes of FE include an intra-osseous infusion, bone marrow harvest and haemoglobinopathies such as sickle cell disease (SCD) 16–18. Among the haemoglobinopathies, SCD is commonly associated with pulmonary consequences. Bone marrow necrosis after vessel occlusion and activation of the clotting system may lead to FE, accounting for 33% of sudden deaths in SCD patients with lung problems 19. Among older patients and those with neurological symptoms, FES often progresses to severe respiratory failure. It has been described after autologous fat harvesting and periurethral injection to treat stress incontinence 20. Other unusual causes include mobilisation of fat in viral hepatitis after pre-existing fatty liver 21, in pancreatitis 22, or from the subcutaneous region due to a liquefying haematoma. Both pulmonary thromboemboli and FE have been found in lethal cases after tumescent liposuction 23. In view of the large number of patients who are treated with liposome-embedded drugs, reports of fatal FE caused by intravenous liposome drug delivery or i.v. hyperalimentation are debatable 24, 25. In lymphangiography (a now largely abandoned examination), FE caused by oily contrast medium injected into the lymph vessels has been reported 26. Occlusion of the lymphatics presumably forced the material to enter veins. Monooctanoin, a mixture of glycerol esters that was used to dissolve gallstones via intrabiliary infusion, has caused deadly fat-like embolisation after i.v. injection 27. Accidental or intentional i.v. lipid overdose has been described after injection of peanut, olive or lamp oil 28. Many preparations intended for intramuscular use only are indeed formulated with vegetable oils. Multiple mineral oil enemas in an infant with Hirschsprung's disease also led to mineral oil embolism 29. Finally, FE has been described following injection of rice bran oil into breasts for the purpose of augmentation mammoplasty 30.
Pathophysiology
The pathophysiology of FES remains largely unclear. Bone particles and fat globules are capable of physically blocking the capillaries of end organs including the lung 5. The observation that the high content of fat in the lungs of injured patients has an identical free fatty acid (FFA) composition to that of bone marrow underlines this theory 31, 32. Small fat droplets may even pass through lung capillaries and enter the systemic circulation 5.
The increase in bone marrow canal pressure during intramedullary instrumentation (e.g. nailing) can lead to “intravasation” of bone contents into the venous circulation 33. The use of conventional cementing techniques is associated with echocardiographic evidence of embolism in 93% of patients 6. The incidence of embolism is reduced with a modified technique that limits intramedullary pressure increases 6. In animal models, a rinsing-suction-reaming procedure developed to lower pressure led to a significant reduction of fat intravasation compared to a universal reamer 34. Intramedullary pressure increases significantly in reamed femoral nailing relative to unreamed 35. Intraoperative prophylactic measures during hip arthroplasty can reduce the incidence of postoperative thrombosis and FE.
Fat globules may enter the systemic circulation through pre-existing precapillary pulmonary or arteriovenous shunts (a patent foramen ovale), which allows showers of systemic emboli leading to obstruction of e.g. brain capillaries. Paradoxical cerebral FE must be considered in the differential diagnosis of altered mental status after fractures or joint replacement, and this condition may even occur despite a lack of a patent foramen ovale or a right-to-left intracardiac shunt 36. Histological features consist of petechial haemorrhages throughout the cortical white matter and, to a lesser extent, the brainstem and spinal cord. It is unknown whether cerebral microemboli after total hip arthroplasty contribute to changes in postoperative cognitive function 37.
Even after a mild skeletal injury, there can be an interval of 24–48 h between the injury and the onset of FES. This delay cannot be explained by mechanical obstruction alone and there is no direct correlation between the amount of fat released and the severity of signs. In the early 1920s, a biochemical theory was introduced 5. Fat emboli may initiate a biochemical and inflammatory cascade. Because pulmonary, renal and subchondral FE and fibrin thromboses are observed, it is suggested that injured marrow adipocytes release fat, thromboplastin and other vasoactive substances that conceivably play a procoagulant role in triggering disseminated intravascular coagulation (DIC). Fat emboli trapped in pulmonary vessels may be metabolised to FFAs and glycerol by lipase secreted by lung parenchymal cells 38. FFAs induce endothelial and pneumocyte damage, capillary leak and clot formation. It is unclear why this cascade occurs in only some patients. Alternatively, circulating FFAs may originate from the breakdown of triglycerides at the fracture site or may become concentrated as a result of systemic lipolysis, induced by circulating catecholamines. The elevation of secretory phospholipase A2 (SPLA2) in patients with an acute chest syndrome in SCD, but not in patients with a vaso-occlusive crisis or non-SCD patients, suggests a role for SPLA2 in FE 39. C-reactive protein may interact with circulating chylomicrons to form fat globules de novo 40. FFAs are also capable of damaging cerebral cortical cells 5. Further evidence for this theory is the observation that exposing neutrophils to oleic acid causes an increase in the cell surface expression and affinity state of the adhesion molecule CD11b, particularly under the acidic conditions that are typical of inflammation 41. This might explain why trauma-induced release of fat causes pulmonary neutrophil accumulation 41. In children, the fat content of the bone narrow is lower, and the composition (less of the toxic oleic acid) is different from that in adults, which might at least partially explain the lower incidence of FE in younger age groups 5.
Clinical signs
The clinical diagnosis of FES is one of exclusion, supported by laboratory and radiological investigations. Gurd 42 and Gurd and Wilson 43 outlined the classical signs and symptoms of FES; diagnosis is based on the presence of at least one of three major symptoms, four of eight minor symptoms and fat macroglobulinaemia. The major signs are respiratory distress, cerebral involvement unrelated to head injury and a petechial rash on the anterior surfaces of the neck, thorax or mucous membranes. The minor features are signs including tachycardia, pyrexia, retinal and urinary changes (anuria, oliguria or fat globules) and laboratory features including anaemia, thrombocytopenia or high erythrocyte sedimentation rate. Remarkably, the inclusion of fat globules in sputum as a minor criterion in the original paper 42 was replaced by jaundice in a second paper by the same group 43. 60% of FES cases present with major symptoms within 24 h with a symptom-free period of at least 6–12 h after the initial trauma 44. 75% of the patients develop pulmonary signs, but respiratory insufficiency requiring mechanical ventilation is rare 45. Hypoxia-related tachypnoea, impaired oxygen diffusion, haemoptysis, combined respiratory and metabolic acidosis, chest pain, cyanosis and hypercapnia are also observed 5. Rales and ronchi may be heard. FE is an indirect cause of ARDS 46.
Central nervous system signs range from encephalopathy to even a comatose state, not improving after correction of hypoxaemia, and may even occur with few or no pulmonary signs 47, 48. Quadriplegia, convulsions and blindness have all been attributed to cerebral FE 49. However, the neurological abnormalities are generally reversible. Fundoscopic evaluation may reveal macular oedema and retinal haemorrhages, and fat droplets may occasionally be seen in the retinal vessels 49. In many cases, petechiae are only discovered after careful inspection of the axillae, the trunk, the neck, the conjunctival sac or oropharyngeal mucosa 8. Petechiae are caused by fat globules that are carried by the bloodstream in the subclavian and carotid artery distributions. Because of their low specific density, fat globules cause petechiae on nondependent, anterior skin areas when the patient is in a recumbent or (semi-) upright position. Skin biopsies have revealed coetaneous extravasations around capillaries blocked by fat and microinfarcts with fat 8. These resolve in 5–7 days.
Diagnosis
Diagnosis is facilitated by the presence of haematological and biochemical abnormalities. Fat globules can be found in blood, urine, sputum, bronchoalveolar lavage (BAL) or even cerebrospinal fluid (fig. 2a⇓). Blood drawn from the femoral vein and examined cytopathologically may yield necrotic bone elements mixed with fat. Pulmonary microvascular cytology consisting of analysis of blood sampled while a Swan–Ganz catheter is in the wedge position has proven to be useful in diagnosing FE(S) 53, 54. However, intravascular lipids can be shown relatively often, although only in patients who have received i.v. lipid emulsions 55. Induced sputum analysis is also a safe and noninvasive test to detect FE in SCD 56.

a) Massive fat embolism syndrome. Bronchoalveolar lavage (BAL) fluid (Oil-red-O staining) showing abundantly present lipid inclusions/fat droplets in alveolar macrophages (original magnification ×400). Reprinted from 50, with permission from the publisher. b) Computed tomography of the chest of a patient with proven fat embolism syndrome showing large ill-defined centrilobular airspace nodules and subpleural nodules (arrows). The nodules are predominantly of ground-glass opacity with some areas of soft tissue attenuation obscuring the edges of the vessels. Reprinted from 50, with permission from the publisher. c) Cytospin preparations (stained according to Papanicolaou's method) of a wedged pulmonary arterial blood sample showing the presence of fetal sqaumae/keratinocytes surrounded by platelets. Reprinted from 51, with permission from the publisher. d) Cytospin preparations (stained according to Papanicolaou's method) of BAL fluid showing fetal sqaumae in a background of inflammatory cells. Reprinted from 52, with permission from the publisher. e) Tumour embolism. Pulmonary artery branch with partially organised embolus containing two acini of adenocarcinoma. Autopsy specimen from a 74-yr-old man with a history of resection of a colonic adenocarcinoma 2 yrs previously (original magnification ×200).
To identify FFAs and fat, cells may be stained with techniques including Oil Red O, Nile blue or Sudan Black staining. The presence of lipid inclusions in alveolar macrophages is associated with various traumatic and nontraumatic conditions, particularly aspiration pneumonia and lipid infusions. BAL Oil Red O-positive macrophages are therefore frequently observed in the BAL fluid of trauma patients irrespective of the presence of FES 57. To define FES, some authors have reported a cut-off of >5% of alveolar macrophages containing fat droplets, ranging 10–100% (median value 46%), in cases with proven or probable FE 58. In another study, bronchoalveolar cells showed many large intracellular fat droplets (mean 63%; range 31–82%), whereas <2% of cells from trauma patients without FE or with non-FE-related ARDS contained such inclusions 59. Others have proposed a threshold of 30% 60. It is conceivable that a high number of Oil Red O-positive macrophages could also reflect clinically silent FE 57. Alternatively, patients with FES showed an increase in the area of fat per alveolar macrophage 61. Thus, automated semiquantitative analysis of fat within macrophages may be helpful in diagnosis but is not routinely available. Recently the most reliable parameter for post-mortem diagnosis was identified as the ratio of embolised tissue area to total tissue area 62. As the presence of fat-containing macrophages in BAL fluid is not specific, serial changes in the percentage of these cells have been suggested to aid in the follow-up of disease severity. The levels of cholesterol (esters) in BAL can be used to distinguish patients with FES from other causes of ARDS. This is related to the activity of enzymes such as SPLA2 and platelet-activating factor (PAF)-acetylhydrolase 63.
In the early stage, atypical radiological findings are bilateral lung infiltrates (chest radiography) or consolidation and ground-glass opacities (computed tomography (CT)). We and others have described the high incidence of small (<1 cm), ill-defined centrilobular and subpleural nodules on CT in the acute phase of FES (fig. 2b⇑). The nodules presumably represent alveolar oedema, micro-haemorrhage and an inflammatory response secondary to ischaemia 50, 64. The dependent distribution of the nodules can be explained by the perfusion-related spread. Ill-defined centrilobular nodules have also been described in patients with acute pulmonary haemorrhage, related to the deposition of haemosiderin-laden macrophages 50. Microhaemorrhages typically occur in FES by the local deposition and metabolisation of FFAs 65. Diffuse lung calcifications located in the branches of the pulmonary arteries have been described in the late course of FES 65. In patients with SCD, areas of ground-glass opacity are identified in segments with hypoperfusion. Denser areas of consolidation reflect either true infarction or infective consolidation 66. Matching defects, especially in the upper half of the lung fields, are seen on ventilation/perfusion 67. Magnetic resonance imaging (MRI) and magnetic resonance-spectroscopy 68 seem to be the most sensitive imaging technique for cerebral emboli, as T2-weighted MRI findings show nonconfluent areas of high intensity in watershed areas. Areas perfused by perforating arteries correlate well with the clinical severity of the brain injury 48, 69. On the diffusion-weighted images, these lesions appear as bright spots on a dark background, a finding known as the “Starfield pattern” 48. Cerebral microembolism can be monitored over time by detecting microembolic signals with transcranial Doppler 70.
Treatment
Treatment of FE should primarily be focused on prevention. Early immobilisation, open reduction and internal fixation of fractures, as well as methods to reduce intramedullary pressure during total hip arthroplasty, have reduced the incidence of FE 5. Early femur fracture fixation (<24 h) is associated with an improved outcome, even in patients with coexistent head and chest trauma 71. Delayed fixation increases the incidence of pulmonary shunting and pneumonia in patients with a high injury severity score and age >50 yrs 72. When fracture stabilisation is delayed in patients with multiple injuries, the incidence of ARDS, FE and pneumonia, the costs of hospital care and the number of days in the intensive care unit (ICU) were increased 72, 73. The exact method of fracture fixation, as opposed to the moment of fixation, plays a minor role in the development of pulmonary dysfunction 10.
FES is largely self-limiting and is usually associated with a good outcome. Current treatments are supportive: adequate oxygenation as well as haemodynamic stability, nutrition and prophylaxis of venous thrombosis and stress-related gastrointestinal bleeding. Therapy follows the same principles as management of ARDS. Transfusions and bronchodilators may improve oxygenation, and most patients who have even severe respiratory failure recover with aggressive treatment 16. Several agents have been used in attempting to reduce the levels of circulating fat, including alcohol, heparin, low molecular weight dextran and aprotinin, but these are not currently recommended. A reduction was shown in the incidence of FES after administration of 10 mg·kg−1 methylprednisolone every 8 h, beginning in the emergency room 74. A beneficial effect of 7.5 mg·kg−1 methylprednisolone given six times hourly for 3 days in patients at risk for FES has been reported 75. However, the true beneficial effect of corticosteroids either before or after the development of symptoms has not been shown in a well-designed trial. High doses of N-acetylcysteine alleviated the pathological changes caused by FE in a rat model 76.
The successful use of veno-venous extracorporeal membrane oxygenation (ECMO) has been reported. ECMO support lasted ∼120 h, followed by an uneventful recovery 77. If a persistent foramen ovale is present, its closure before surgical manipulation of the fracture is feasible 78.
AMNIOTIC FLUID EMBOLISM
Although entry of amniotic fluid (AF) into the maternal circulation was first reported in 1926, it was not until 1941 that the importance of the condition was emphasised 79. The presence of fetal debris in the pulmonary vessels of females who died during the peripartum period was then reported 80.
Incidence
The incidence of AF embolism (AFE) ranges 1 in 6,000–120,000 pregnancies 81–84. AFE usually occurs during the immediate postpartum period 85. Analysis of a national registry revealed that AFE occurred during labour but before delivery in 70% of cases and during caesarean section in 19% 86. AFE has been reported as early as the second trimester. The diagnosis in cases occurring as late as 36 h postpartum is, however, debatable 87. AFE following transabdominal amniocentesis is very rare 88. Estimates emphasise that AFE has accounted for 12% of all maternal deaths related to legally induced abortion since 1972, with a death-to-case rate of 0.2 per 100,000 abortions 89, 90. AFE is seldom associated with (surgical) manipulation during caesarean section 91, curettage 92, cervical suture removal 93 or repair of an incompetent cervix 93, or after car or motor vehicle accidents 94. The 24 well-documented cases of AFE occurrence following (surgical) trauma have been recently reviewed 52. At least 13 of these patients died of causes directly related to AFE 52.
Originally suggested 80 predisposing factors, such as advanced maternal age, multiparity and tumultuous labour, could not be identified by others 81, 86. A large fetal size, use of oxytocics and vaginal prostaglandins, advanced gestational age, amnioinfusion or complicated labour have all been implicated 81, 95. In reality, specific risk factors have not yet been conclusively identified. Logistic regression identified advanced maternal age, placental pathologies and caesarean deliveries in a large population-based cohort study 96. The reported case fatality rate continues to be high: it might account for 10% of all maternal deaths in the USA. In the registry by Clark et al. 86, the mortality was 61%; in a recent cohort study it was 21.6% 96. There were only 39 survivors in another series of 272 cases, which indicates a mortality rate of 86% 81. Among the survivors in the registry of Clark et al. 86, only 15% were neurologically intact. All deaths occurred within 5 h of collapse, depending on the duration of resuscitation efforts. In a population-based study, maternal mortality rate (26.4%) was less than previously reported and might reflect a more accurate population frequency 84. Of the 31 survivors of a UK registry, 12 women experienced cardiac arrest. Of the 13 women who died, seven of their babies survived 83. Although there is still significant maternal and neonatal morbidity, the vast majority of women will nowadays survive 83.
Pathophysiology
The pathophysiological mechanism of AFE is poorly understood 82, 85. Previous theories stated that the infusion of AF into the circulation occurred after tumultuous labour 80. With the evidence available today, these theories are indefensible. AFE may be related to the infusion of abnormal AF. Finding epithelial squames from the fetal skin in the pulmonary artery (PA) alone is not pathognomonic; rather, the combination of symptoms with detection of these cells is required 85. Furthermore, there is not a clear temporal relationship between the entry of AF into the maternal circulation and symptom onset. AF may routinely enter the maternal circulation during delivery through open veins of the placenta or via tears in the lower uterus or cervix. Proposed mechanisms therefore include not only mechanical obstruction of the pulmonary vasculature by amniotic debris but also a reaction similar to septic shock 85. The apparently idiosyncratic nature of the response and the presence of antigenic factors in AF has led some authors to propose AFE as an “anaphylactoid syndrome of pregnancy” 85. This term implies that the severity of symptoms is related to the host reaction to a foreign antigen, driven by the antigenic potential of the AF. If AF composition determines this reaction, this might explain why women carrying a male fetus tend to be more frequently affected 86. Similarly, meconium-stained AF may be more toxic than clear fluid.
AF is a complex mixture of maternal extracellular fluid and fetal urine, squamous cells, lanugo hairs, vernix caseosa, mucin and sometimes meconium 79. Particulate matter originating from the AF has been identified at autopsy in the lung, kidney, liver, spleen, pancreas, brain and even retina 97, 98. AF has no direct effect on the isolated human omental artery. The haemodynamic changes associated with AFE may therefore be due to secondary responses 99. During labour, significant concentrations of prostaglandins appear. Other humoral factors, including proteolytic enzymes, complement factors, PAF, histamine, serotonin and leukotrienes, may contribute to the haemodynamic changes and consumptive coagulopathy associated with AFE. At autopsy, the pathological changes usually associated with DIC can be found in the many organs. Eosinophilic infiltrates have been reported in the lungs, hepatic portal fields and the heart, strengthening the theory of a hypersensitivity reaction 100. Antitryptase staining of pulmonary tissue has revealed massive mast cell degranulation 101, 102. Elevated serum levels of the neutral mast cell-derived protease tryptase add further supporting evidence for mast cell degranulation 103. A numerical increase of pulmonary mast cells is seen in subjects who died of AFE, with values that correspond to those encountered in deaths due to anaphylaxis 101. Serum tryptase and urinary histamine measurements were negative in another series but most women with AFE had elevated levels of fetal antigen 104.
Isolated DIC may be the first indication of AFE 105. AF accelerates clot initiation and propagation. When AF is added to blood from pregnant women, the R time, which reflects the time to first clot formation, is significantly decreased with the addition of as little as 10 μL to 330 μL blood. This substantiates the hypothesis that coagulation profile changes are invariable accompaniments of AFE 106. The Thrombelastograph® test may therefore be useful in assessing coagulopathy during or after AFE 107. AF also contains large amounts of tissue factor (TF) pathway inhibitor (TFPI), accounting for virtually all of its coagulant potential. The intrusion of AF into the bloodstream may influence the plasmatic TFPI–TF equilibrium, which also results in DIC 108. Isolated rat hearts perfused with varying concentrations of human AF also experience a dose-dependent decrease in coronary flow rate, rather than directly suppressing myocardial activity 109. Several factors activated by AF have been shown to depress cardiac function 110.
Clinical signs
The condition can be neither predicted nor prevented. Probably the best diagnostic criteria focus on the constellation of signs and symptoms published in 1974 111. This was recently proposed in a slightly modified form: 1) currently pregnant or within 48 h of delivery; 2) one or more of the following observations severe enough to require medical treatment: a) hypotension; b) respiratory distress; c) DIC; or d) coma and/or seizures; and 3) absence of other medical explanations for the dramatic clinical course 112. The presentation of AFE can be quite variable with respect to timing, symptoms and subsequent course: sudden onset of hypoxaemia and cardiovascular collapse are the main symptoms. These are often preceded by agitation, nausea or seizures. In 51% of cases, the presenting symptom is respiratory distress and isolated respiratory failure has been reported 105. In the remainder, the first signal is hypotension (27%), coagulopathy (12%) or seizures (10%) 81. Disturbances of coagulation, ranging from mild thrombocytopenia to overt DIC or isolated DIC without cardioplumonary instability, have been described. Two pregnancy-specific conditions of NTPE (choriocarcinoma and AFE) are rarely responsible for focal cerebral ischaemia, but global encephalopathy is not uncommon. A majority of AFE patients develop seizures and permanent neurological sequelae 85, due to impaired oxygen delivery to the brain 113.
Some patients are diagnosed with pulmonary oedema 51, 114, 115 and ARDS later in the course of the disease. Until recently, it was believed that the major haemodynamic change in AFE was the development of severe pulmonary hypertension due to critical obstruction and vasospasm of the pulmonary vessels, as suggested in animal models. Several reports suggest, however, the presence of severe transient left ventricular failure. PA catheter readings in human AFE cases frequently show low cardiac output and elevated pulmonary capillary wedge pressure as well as low left ventricular stroke work index 51. A biphasic pattern of haemodynamic changes has therefore been postulated to reconcile the data, in which a first transient period of cor pulmonale exists, followed by left heart failure 115. There are no clear human data confirming this biphasic pattern. In 1990, the haemodynamic data were reviewed indicating that left ventricular dysfunction was present with secondary mild-to-moderate increase in PA pressure in all available cases 85. We recently reviewed all 18 well-documented cases of left ventricular failure after AFE. In five out of these 18 reported courses, the left ventricular failure contributed to the fatal course 51.
Diagnosis
AFE is again a diagnosis of exclusion. Identification of squamous cells in the maternal pulmonary arterial circulation, either at autopsy or intra vitam, was originally regarded as pathognomonic (fig. 2c⇑) 51. Finding fetal elements in the PA can only be considered supportive. Squamous cells can appear in the pulmonary blood of heterogeneous populations of pregnant and nonpregnant patients 115, also resulting from contamination by exogenous sources during specimen preparation or derived from the entry site of the PA catheter 116. Trophoblastic cells are free-floating in the intervillous space and have direct access to the maternal circulation. Therefore, blood from the PA should be collected as described by Masson and Ruggieri 117 and Masson 118. In order to minimise the possibility of contamination, a representative sample could be obtained if blood is drawn from the distal lumen of a wedged PA catheter. After discarding the first 10 mL, an additional 10 mL is drawn, heparinised and analysed utilising Papanicolaou's method 119. Reliable differentiation of adult from fetal squamous cells is not possible; however, the significant increase in cell count documented in pregnant patients suggests a possible fetal origin for some squamous cells detected during pregnancy. In a critically ill obstetric patient, squamous cells in the pulmonary vessels should not deter the clinician from a search for other causes of instability 115.
Squamous cells coated with neutrophils or thrombocytes, accompanied by fetal debris, or eosinophilic granular material with adherent leukocytes are considered more likely to be found in AFE (fig. 2c⇑) 117, 120. The diagnosis may be further supported by the presence of amniotic cells in BAL fluid (fig. 2d⇑) 52. Rhodamine B fluorescence may identity sparsely distributed fetal squames that otherwise may be overlooked by less sensitive tinctorial methods 121. Detecting the simultaneous presence of syncytiotrophoblast cells and megakaryocytes in the pulmonary microvasculature by means of a panel of monoclonal (CD61-GpIIIa, beta-hCG) and polyclonal (FVIII-vW, hPL) antibodies allowed the confirmation of AFE 122. The staining of fetal isoantigen or staining with an antibody raised to human keratin have all been described 123. Immunohistochemical staining with the sensitive monoclonal antibody TKH-2 against a common fetal antigen (Sialyl Tn, NeuAc alpha 2-6GalNAc) had a high sensitivity for diagnosing AFE 124. AFE can indeed be easily missed on haematoxylin and eosin sections. As Alcian blue staining may also be insufficient to show intravascular mucin in the maternal lung sections, TKH-2 immunostaining is a more sensitive method to detect AF-derived mucin in lung sections 125. Measuring zinc coproporphyrin I, a characteristic fetal-gut component of meconium, in maternal plasma may be a sensitive method to diagnose AFE 126.
Chest radiography reveals diffuse bilateral homogeneous opacities 2. Because AFE is characterised by the absence of frank pulmonary vessel obstruction, it has only been occasionally reported to present with the obstruction of branches of the PA during angiography 127. Transoesophageal echocardiography may reveal enlargement of the right ventricle and main pulmonary trunk, consistent with acute right ventricular pressure overload, but also full-blown left ventricular failure in view of the depression of left ventricular function 51.
Treatment
AFE can be neither predicted nor prevented so randomised controlled trials are not possible. The maternal and fetal outcome is unpredictable. The majority of patients will require ICU admission 113. Management is directed towards the maintenance of oxygenation, circulatory support and correction of the coagulopathy. Mechanical ventilation can be necessary to maintain oxygen supply as well as invasive monitoring to guide the use of inotropic agents and fluid. Optimisation of cardiac preload by volume expansion in hypotension and inotropic support is indicated if (left) heart failure is observed 51, 114. In some cases, after-load reduction may be beneficial in restoring cardiac output, providing pre-load is adequately preserved. Diuretics are useful to mobilise pulmonary oedema.
In 65% of AFE cases, delivery had not yet occurred. Immediate delivery of the fetus by caesarean section is mandatory to prevent fetal hypoxic damage and facilitate resuscitation 82. Case reports have highlighted the importance of displacing the uterus laterally to avoid compressing large vessels and even performing an emergency caesarean section during resuscitation 128. Treating the coagulopathy involves the administration of blood components. Cryoprecipitate is rich in fibronectin, which aids the reticulo-endothelial system in the filtration of antigenic matter. Historically, depleted levels of this glycoprotein have been reported, with improvement following repletion of fibronectin levels 129. The successful use of activated recombinant factor VIIa in the management of severe haemorrhage secondary to AFE has been reported 130. Leukocyte depletion filtering of cell-salvaged blood obtained from caesarean section might reduce particulate contaminants to a concentration equivalent to maternal venous blood 131. Several studies have revealed no increased risk of complications after autologous blood autotransfusion during caesarean section.
Novel therapies have been described anecdotally. Successful haemorrhage management may be further optimised by uterine artery embolisation, thus avoiding hysterectomy 132. Plasma exchange transfusions, continuous haemofiltration and aprotinin administration have been attempted 86, 133, as has the use of nitric oxide or inhaled aerosolised prostacyclin to treat hypoxaemia 134, 135. In light of the similarities to anaphylaxis, corticosteroids and epinephrine have been suggested as useful therapeutic adjuvants 86. ECMO and intra-aortic balloon counterpulsation might be considered in left ventricular failure unresponsive to medical therapy 136. The successful treatment of a moribund patient with cardiopulmonary bypass and PA thromboembolectomy has also been shown 137.
TUMOUR EMBOLISM
The lung is a target of remote malignancy: embolism to the pulmonary vasculature is obviously a prerequisite for the development of metastasis but has rarely been described as a distinct entity. Pulmonary tumour embolism (PTUE), characterised by the occlusion of pulmonary vessels by tumour cells, was described more than 100 years ago 138. It was not until 1937 that cor pulmonale due to emboli to the pulmonary microvasculature was described 139.
Incidence
Macroscopic PTUE has been reported in sarcomas, hepatocellular, breast and renal cell carcinomas, whereas microscopic PTUE was found predominantly in gastric, hepatocellular and pancreatic carcinomas and choriocarcinomas It has also been described in patients with lung, prostate, thymic, gall bladder, bladder, colorectal, skin or cervical cancer 140–143. Pulmonary hypertension may be seen occasionally as a consequence of capillary plugging by malignant megakaryocytes in essential thrombocytopenia. Tumour emboli might occur subclinically and were seen microscopically in 2.4–26.0% of autopsies of patients with a solid malignancy 144–147. In a review of 1,069 autopsies, three cases in which death had occurred from cor pulmonale due to tumour embolisation from breast, lung, and ovarian carcinoma were observed 148. Tumour macroembolism is also reported in the setting of sudden death requiring medicolegal investigation 149. It should be distinguished from primary tumours arising from the intima of the PA, such as malignant fibrous histocytoma or sarcoma 150.
Pathophysiology
Macroembolism is a feature of primary tumour sites that are connected by the vena cava to the right ventricle 151. Tumour emboli possess an unusual level of resistance to recannulation and are therefore more likely to lead to progressive, irreversible obstruction. Most cases of microembolism show a vascular tissue reaction with intimal proliferation and fibrosis (fig. 2e⇑); bland tumour emboli without or with only scarce vascular reaction are rarely seen 140, 152. In PTUE, anywhere from 7–81% of the pulmonary arteries contain emboli 147. The extent of the occluded cross-sectional area of the pulmonary arterial bed determines the increase in pulmonary vascular resistance and explains why only some patients become symptomatic. There is usually no marked cardiopulmonary functional derangement until 60–80% of the pulmonary arterial bed has been occluded. At some degree of obstruction, the ability of the pulmonary vasculature to adapt is impaired 153.
Platelets and thrombin are frequently present in addition to malignant cells. As organisation of the thrombus occurs, the embolic cancer cells degenerate. Fibrocellular intimal hyperplasia and fibrosis of pulmonary arteries may occur with smooth muscle colonisation of the luminal neoplastic lesions, both adjacent to emboli and in vessels where emboli are not seen 145, 154. PTUE is different from a haematogenous, true metastasis, as there is no tendency for the tumour emboli to invade the arterial wall 141, 146. Tumour emboli are destroyed or remain latent intraluminally 141. The eventual outcome of malignant cells in the lung (metastasis, invasion of lymphatics, development of pulmonary hypertension or clearance of the cells) is the result of interactions between signalling pathways that affect angiogenesis, apoptosis and inflammation. Necropsy series 146, 147 suggest that there are four types of pulmonary involvement: 1) large tumour emboli occlude the pulmonary arteries; 2) microscopic tumour emboli involving the small vessels account for subacute pulmonary hypertension found in the majority of cases; 3) pulmonary microvascular invasion may be part of the generalised lymphatic involvement, which explains the diffuse interstitial infiltrates seen in some cases; and 4) pulmonary tumour embolism can be caused by a combination of the above mechanisms 141, 153.
Clinical signs
Pulmonary tumour microembolism may be suspected in patients who complain of unexplained dyspnoea and develop cor pulmonale. The most common symptom is subacute progressive dyspnoea which occurs in 57–100% of cases over a span of weeks to months 141, 147, 153, as well as pleuritic chest pain, cough, haemoptysis and weight loss 2. In a retrospective review of 164 cases, a typical profile of features was reported: documented or suspected underlying malignancy, acute-to-subacute onset of dyspnoea and signs of cor pulmonale 141. Retrospective chart reviews demonstrate that only 8% of patients with pathological evidence for PTUE have documented morbidity or mortality attributable to the emboli: the “classic,” signs of right heart failure are reported in only 15–20% of patients 148, 155.
Arterial blood gas measurements invariably show hypoxia, usually hypocapnia or increased alveolar–arterial oxygen gradient 141. In many instances, metastases to other organs were documented prior to the onset of respiratory symptoms. However, PTUE as the initial manifestation of underlying malignancy was also reported in a few patients 141.
Diagnosis
Tumour macroembolism is clinically indistinguishable from thromboembolism, and the diagnosis is therefore achieved mostly through autopsy 140. The presence of both thrombotic and tumour PE should be considered in all cancer patients because of similarities 156. Even in patients known to have a malignancy, the correct diagnosis is made in as few as 6% ante mortem 145. Moreover, PTUE has a lack of specific radiological features and mimics pneumonia or interstitial lung disease. A normal chest radiograph with hypoxaemia in a patient with a malignancy might even suggest the presence of PTUE: only one out of eight patients had a parenchymal abnormality on a plain radiograph 147. Cardiomegaly and prominent pulmonary vasculature, the radiographic changes associated with elevated pulmonary pressures, are seen in <50%. In an attempt to distinguish carcinomatosis and tumour emboli, some investigators suggest that lymphatic disease is more likely to have an interstitial infiltrate.
Subsegmental, mismatched peripheral defects have been described on ventilation–perfusion in patients with exclusively microvascular disease 157. The ventilation scan is usually normal 141. Tumour emboli are usually located in small or medium arteries so angiography, the gold standard for thromboembolic disease, has poor sensitivity and specificity for detection: “typical” pulmonary angiographic findings include delayed filling of the segmental arteries, pruning and tortuosity of the third- to fifth-order vessels. The CT findings further include multifocal dilatation and beading of the peripheral subsegmental arteries and peripheral wedge-shaped areas of attenuation due to infarction 158. However, most patients have no evidence of embolic disease by pulmonary angiogram 159. The tree-in-bud pattern is commonly seen on thin-section CT of the lungs, and it consists of small centrilobular nodules of soft tissue attenuation connected to multiple branching linear structures of small calibre that originate from a single stalk 160. Originally described in cases of endobronchial spread of Mycobacterium tuberculosis, it is now also recognised as a manifestation of PTUE 161.
The use of transoesophageal echocardiography, accurately defining the cephalad extent of the thrombus, might be considered in diagnosing and guiding intraoperative management of a migratory embolus from the inferior vena cava. Radiolabelled monoclonal antibody imaging and repeated pulmonary microvascular cytology sampling techniques were historically promising diagnostic tests 141. Obtaining a suitable sample of blood from the pulmonary capillary bed for tumour cells again requires that blood be aspirated from the distal port while the catheter is in the wedged position to avoid malignant cells from “upstream” (e.g. the liver) contaminating the sample. Blood is subsequently either filtered or spun down, and the remaining cells stained with the Papanicolaou method. The interpretation of such samples proves to be challenging, as megakaryocytes and endothelial cells may mimic malignancy 162.
Treatment
The prognosis is poor and the median survival from diagnosis is a few weeks. In view of these patients' likely prognosis, interventions to cure or slow down the progressive deterioration are rarely performed. The principal intervention in most cases was surgical resection of the primary neoplasm, if possible. Surgical cure by resection of the primary tumour has been reported in patients with atrial myxoma, renal cell carcinoma and choriocarcinoma 141. Chemotherapy is rarely indicated, although favourable results have also been reported in patients with choriocarcinoma and breast cancer 159.
TROPHOBLASTIC MATERIAL FROM GESTATIONAL TROPHOBLASTIC DISEASE
Incidence
Gestational trophoblastic disease (GTD) defines a heterogeneous group of inter-related lesions arising from abnormal proliferation of the trophoblastic epithelium of the placenta. Two subtypes arise from an aberrant fertilisation (complete or partial hydatiform mole) and three malignant subtypes (invasive mole, choriocarcinoma and placental site trophoblastic tumours) may occur after any gestational experience 163. Trophoblastic embolism may be subclinical in normal pregnancy and more pronounced in eclampsia. It also occurs within hours following abdominal hysterectomy for invasive moles, molar evacuation and as a side effect of chemotherapy for choriocarcinoma 164–166.
Pathophysiology
The pathogenesis is unique because the tumour arises from fetal, not maternal, tissue. The question has been raised whether trophoblastic embolisation is an entity that occurs independent of pulmonary oedema (a sequel of accompanying hyperthyroidism), pre-eclampsia and fluid overload or whether discovery of trophoblastic tissue in the lungs is merely coincidental 167. Even when a mass of molar tissue is gently manipulated, there is a risk of pulmonary trophoblastic emboli. On the other hand, although multinucleated giant cells and large mononuclear cells are identified in the buffy coat of blood aspirated before and during evacuation of large molar pregnancies, no significant changes in mean systemic arterial, pulmonary arterial or capillary wedge pressures were seen. Likewise, cardiac output and pulmonary vascular resistance were mostly unchanged. When significant decreases in haemodynamic variables were observed during evacuation, these returned to pre-evacuation levels after completion of anaesthesia 164. This indicates that trophoblastic embolisation sufficient to cause severe pulmonary compromise is rare.
Clinical signs
Vaginal bleeding is the most frequent symptom of GTD. Self-limited respiratory distress arises in 3–10% following molar evacuation, with the number rising to 25% when the uterus is larger than predicted for the gestational age and the human chorionic gonadotropin level exceeds 100,000 mIU·mL−1 168. The acute illness, which requires aggressive support, lasts 24–48 h. This is typically followed by a dramatic clinical improvement over the following 48–96 h, with pulmonary function returning to baseline generally within 72 h 168. Due to the routine use of ultrasound and beta-hCG in the workup of early gestational abnormalities, complete molar pregnancy rarely presents today with the traditional signs although the potential for persistent trophoblastic disease still exists 169. Pulmonary trophoblastic embolism is infrequently associated with sudden death 166, 170.
Diagnosis
Pulmonary involvement occurs in up to 80% of women with metastatic GTD 171. Radiographic findings are variable and include alveolar, nodular and miliary patterns, pleural effusion and signs of pulmonary arterial occlusion 165. Again, some authors have demonstrated syncytiotrophoblast and multinucleated trophoblastic giant cells in pulmonary arterial blood sampled during molar evacuation 164, 172.
Treatment
Management of trophoblastic embolisation is no different from that of other causes of hypoxaemia and NTPE. Infusions of fluid and blood tend then to cause pulmonary overload, which may precipitate heart failure. Preferred therapy consists of diuresis and ventilatory support 167. Emergency pulmonary embolectomy under cardiopulmonary bypass has been reported for an embolism of malignant trophoblastic material 173.
SEPTIC EMBOLI
Incidence
Septic pulmonary embolisation (SPE) is a rare but well-recognised problem in the setting of right-sided endocarditis and septic thrombophlebitis from such sources as the tonsils, the jugular, dental or pelvic region and infected central venous catheters 174, 175. SPE is becoming an uncommon complication of i.v. drug use, presumably due to greater needle hygiene 176. The increasing use of long-term indwelling catheters or prosthetic vascular devices as well as increasing numbers of immunocompromised patients have changed the epidemiology 176. In children too, soft tissue infection, osteomyelitis and i.v. catheters have been recognised as risk factors 177.
In a huge series of post-mortem examinations in Japan, SPE was found in 2.2% of 11,367 cases of “critical” pulmonary embolism 178. Infectious endocarditis was responsible for 11% of these cases of SPE. Surprisingly, fungal emboli (from Aspergillus, Mucor or Candida) were found more frequently than bacterial: most of these fungal emboli had a (haematological) malignancy as the underlying risk factor 178. This is in contrast with a low incidence of reported cases of Aspergillus tricuspid endocarditis 179.
A peculiar subtype is Lemierre's syndrome (postanginal sepsis), an anaerobic thrombophlebitis of the internal jugular vein with metastatic infection. Most patients affected are young adults with tonsillopharyngitis, odontogenic infection, mastoiditis or sinusitis. The causative organisms include the anaerobic gram-negative Fusobacterium species, but also Eikenella, Porphyromonas, Streptococci and Bacteroides 180, 181. Recently, methicillin-resistant Staphylococcus aureus has been identified as a new causative agent 182. Extension of the infection to the adjacent lateral pharyngeal tissue results in haematogenous spread. Pulmonary involvement in Lemierre's syndrome has been reported in up to 97% with lung abscesses and empyema 183.
Pathophysiology
Septic pulmonary emboli reach the lung from many sources, including infected heart valves, thrombophlebitis and infected catheters or pacemaker wires 180, 184. In tricuspid endocarditis, local infection can produce typical cystic lesions, often complicated by empyema. A thrombus containing microorganisms embedded in fibrin mobilised from an infectious nidus is implanted in the pulmonary arteries, leading to an infarction inciting a metastatic abscess (fig. 3a⇓) 176, 185. Cavitary parenchymal nodules may be caused by septic occlusion of small peripheral PA branches 186. Pulmonary infarction is uncommon when the emboli obstruct the central arteries but is frequent when distal arteries are occluded 187. This may be explained by collateral flow from the bronchial arterial circulation that enters the PA distal to the site of an obstruction 186. Peripheral parenchymal consolidation (wedge-shaped lesions) is then partially caused by pulmonary haemorrhage from the extravasations of the bronchial arterial flow 188.

Septic embolism. Lung infarction by a septic thrombus from the tricuspid valve in a 21-yr-old female with endocarditis. Repeated blood cultures and culture of the valve disclosed a positive culture for Staphylococcus aureus. a) A haematoxylin- and eosin-stained section of this infarcted lung specimen shows the obstructed large pulmonary artery branch and surrounding lung tissue with coagulation necrosis (original magnification ×40). b) Chest computed tomography of this patient with endocarditis of the tricuspidal valve and pulmonary septic emboli. Axial computed tomography showing multiple irregular nodules of which some are cavitated. Moreover, feeding vessels are demonstrated leading directly to a subpleural cavitated nodule in the right upper lobe (white arrow).
Clinical signs
The characteristic features are a febrile illness, cough, haemoptysis and lung infiltrates associated with an active focus of extrapulmonary infection 176, 189.
Diagnosis
Clinical and radiological features at presentation are nonspecific, and the diagnosis is frequently delayed 176. Blood cultures, chest CT and echocardiography are invaluable when evaluating a patient with suspected SPE 176. Transoeasophageal echocardiography provides greater spatial resolution compared with transthoracic imaging and is a superior method for imaging vegetations, abscesses and leaflet perforations 190. Typical radiographic features include patchy air space lesions simulating nonspecific bronchopneumonia, multiple ill-defined round or wedge-shaped densities of varying sizes located peripherally and lesions abutting the pleura and located at the end of vessels (feeding vessel sign) scans 177, 184 (fig. 3b⇑). This feeding vessel sign has also been reported in both uncomplicated pulmonary emboli and pulmonary metastases and simply indicates the haematogenous origin of the parenchymal nodule 184, 191. Transverse images showed that 37% of the nodules and 22% of the wedge-shaped opacities in SPE had a vessel that appeared to enter the nodule, although both multiplanar reconstructions and maximum-intensity projections showed that the vessels passed around the nodules 191. All of these vessels were traced to the left atrium, a finding consistent with pulmonary vein branches 191. Multi-detector CT is superior to the classical CT technology for detection of this feeding sign. Rapid progression of the lesions to cavities or abscess formations can occur 177.
It is noteworthy that Kwon et al. 185 recently reported that the size of the nodules in gram-positive septic emboli was larger than those in gram-negative. Cavitation and air bronchogram within the nodules were seen more frequently in the gram-positive emboli, while a ground-glass attenuation halo around a nodule and a feeding vessel sign were more commonly observed in gram-negative emboli. Hemorrhagic nodules have a characteristic, although nonspecific, CT appearance that consists of a central area of soft tissue attenuation surrounded by a halo of ground-glass attenuation, termed the CT “halo” sign. This sign can be caused by several pathological processes and is found in haemorrhagic pulmonary nodules as well as nonhaemorrhagic inflammatory lesions 192, 193.
Treatment
Septic patients are also at risk of thrombotic pulmonary embolism 194. The management of a free-floating (even septic) thrombus in the femoropopliteal or iliocaval veins is therefore controversial. Although the deployment of inferior venal caval filters is of theoretical benefit, the uncertainty of their potential adverse event profile has limited their current use. Although debated 194, it is usually proposed that venal caval filters should not be implanted in patients with risk of septic embolism. 195.
In 1978, MacMillan et al. 189 described 60 patients with SPE: i.v. drug users comprised 78% of their cohort, and tricuspid endocarditis was the embolic source in 53%. At that time, 20% still required thoracotomies to manage lung abscess, bronchopleural fistula and empyema 189. Recent studies demonstrate improved outcomes for patients with SPE with virtually all patients recovering from their illness. This may be attributable to earlier diagnosis, prompt administration of broad-spectrum antibiotics and improvements in surgical and supportive care 176, 196. High doses of i.v. antibiotics targeting anaerobic organisms in Lemierre's syndrome are indicated 197.
HYDATID CYSTS
Incidence
Cystic hydatid disease or echinococcosis is a parasitic infection caused by the larval or cyst stage of the tapeworm Echinococcus granulosus. Humans can be infected by ingesting eggs, from which cysts develop in the liver and lung. Echinococcosis is mostly endemic in sheep-farming areas of the Middle East, South America, Oceania and along the Mediterranean coast 198.
Pathophysiology
The parasite can reach any part of the body, although the organs most commonly affected are the liver (75%) and lungs (15%) 199. The embryo rarely reaches the right heart cavities through the portal or lymphatic routes. Hydatic PE occurs after rupture of a hydatid cyst in the right ventricle or atrium, or more rarely haematogenous dissemination from a hepatic focus rupturing into the hepatic veins or the inferior vena cava 200, 201. Autopsy findings indicate that embolism is caused by vesicles or cysts that act purely mechanically by obstructing the blood flow, as there are no blood clots or added thrombosis 202. Hydatid cysts may rarely present in the wall of the arteries 200, 201.
Clinical signs
The major complication is rupture of the cyst into the pericardium, which can lead to anaphylactic shock or tamponade 200. The clinical manifestations of pulmonary arterial hydatid cyst embolisation are not specific, although haemoptysis is the most frequent sign 203, 204. It is classified according to the clinical presentation: 1) acute fatal cases; 2) subacute pulmonary hypertension with death in less than a year; and 3) chronic pulmonary hypertension 3. The majority of cases appear to follow a course of prolonged pulmonary hypertension punctuated by acute embolic episodes 204, 205. A cardiac hydatid cyst that caused complete occlusion of the right PA has been described 205. Seldomly, a primary interventricular cyst may rupture via the pulmonary veins, resulting in multifocal pulmonary cystic lesions 206.
Diagnosis
The diagnosis is difficult in the absence of typical clinical and radiological findings. Serological tests, though more specific than imaging techniques, are less sensititve but are useful confirmatory tests 207. Diagnosis, guided by echocardiographic findings, is mostly based on the arteriogram, revealing segmental or lobar perfusion defects 208. Some authors have emphasised the role of combined contrast-enhanced spiral CT, MRI and pulmonary magnetic resonance angiography of the chest to evaluate complicated cardiac hydatid cysts. Echinococcal embolisation to the PA has also been studied with these techniques in the absence of intracardiac and hepatic hydatid cysts 203. On enhanced CT, the intra-arterial cyst shows a typical hypodense appearance 203.
Treatment
When a right-sided cardiac hydatid cyst is diagnosed, early surgical treatment should be performed under open-heart surgery conditions 198. Median sternotomy and the use of extracorporeal circulation must be the surgical approach of choice when cysts are present in the cardiac chambers 202. Embolectomy by removing multiple fragments of a ruptured endocyst of the PA, followed by surgical closure of the cardiac cyst cavity, can be performed 209. Surgical intervention can be complicated by rupture of the artery and/or the cyst. Dissemination of the disease, anaphylactic shock and pseudoaneurysm formation can then occur 203. Surgical treatment combined with chemotherapy may improve the prognosis 200. Medical therapy is advocated for patients with recurrent hydatidosis or in those where surgical intervention involves a high risk. This poor prognosis depends on the patient's general status as well as the number and size of the embolised vessels.
PARTICULATE MATERIAL
Incidence
The i.v. injection of illicit drugs or drugs intended for oral administration is associated with a variety of pulmonary consequences. Some of these oral medications, including amphetamines, methylphenidate, methadone, meperidine, pentazocine, hydromorphone and dextropropoxyphene, are ground by drug users, mixed in liquid and then injected intravenously 210, 211. The i.v. abuse of pharmaceuticals such as codeine and temazepam has also been reported 212.
Other emboli-causing substances including talcum, starch, cellulose and cotton may be observed in individuals who engage in i.v. drug abuse or parenteral injection of these tablets. Substances such as magnesium trisilicate, corn starch and microcrystalline cellulose are used as fillers and binders during manufacturing 213. Pills, containing both active drug and fillers, are crushed and dissolved in water by heating the mixture. This solution is drawn into a syringe using cotton as a filter before injection. When the supply of available drug is exhausted, addicts may heat the cotton balls in water to draw any trapped drug back into solution 210. Similar emboli can also occur in the hospital when cotton fibres remain on angiographic guide wires or catheters after they have been wiped with moist cotton gauze 214. The nature of the material in lung tissue from 33 addicts appeared to be birefringent material in 31 cases, with talcum being the only material in eight cases or in conjunction with other materials in all remaining cases 215. Crospovidone, an insoluble polymer used as a disintegrant, can also embolise when tablet suspensions are injected 216.
Catheter emboli are rare iatrogenic complications as they usually develop when a physician attempts to withdraw a catheter through an introducing needle. The catheter catches on the needle, and the distal portion is sheared off. Spontaneous catheter breakage accounts for 25% of catheter emboli. Most catheter emboli are found in the basilic vein and the pulmonary arteries, with the remainder in the right heart, great veins and peripheral lungs 217. Cannulation of antecubital, subclavian, femoral and internal jugular veins, as well as cardiac catheterisation and temporary pacemaker insertion have all been associated with embolisation 218. Central embolisation of needle fragments has also been reported in i.v. drug abusers 218.
A great variety of materials can embolise. Teflon from an eroded valve has been found in the vessel walls and parenchyma of the lung 219. Pulmonary emboli caused by accidental or intentional i.v. injection of metallic mercury (fig. 4⇓) have been encountered 3, 220. Liquid silicone, an inert material used for medical purposes but also during illegal cosmetic procedures in women and transsexual men, may embolise 221. Patients with arterio-venous malformation (AVM) undergo endovascular treatment with embolisation of different materials, including cyano-acrylate agents, polyvinyl alcohol foam particles, microcoils, silk or dacron thread and balloons 222. Three out of 182 patients who had undergone embolisation of brain AVMs with cyano-acrylate, developed pulmonary symptoms due to embolisation within 48 h of the procedure 223. Although percutaneous vertebroplasty is usually safe, symptomatic pulmonary embolisation of acrylic cement used during this procedure has been described (fig. 5⇓) 224.

Chest radiograph of a male who presented at the emergency room after the intravenous injection of mercury during a suicide attempt. Note the small metallic spherules scattered throughout both lungs. Recognition of metallic opacities in the heart allows differentiation from aspiration.

Polymethylmethacrylate embolism as an incidental finding after a history of percutaneous vertebroplasty. Axial computed tomography of a) the mediastinal and b) the pulmonary window shows a linear hyperdensity in a pulmonary artery branch (white arrow).
Prostate brachytherapy, achieved by image-guided placement of radioactive seed implants carrying iodine-125 or palladium-103 in the prostate and periprostatic tissues, is a therapeutic option for patients with localised prostate cancer. These implants may detach from their insertion sites and migrate through the prominent periglandular or haemorrhoidal venous plexus to reach the pulmonary circulation 225. The frequency of seed implant migration ranges from 0.7–55% 226, with an average of 2.2 embolised seeds per patient. Proper identification of periprostatic vessels and the use of individualised applicators have lowered the incidence of seed embolisation 227.
Pathophysiology
Talcum-induced pulmonary granulomatosis has an unknown physiopathological mechanism, although the most likely hypothesis is an immunological mechanism of delayed hypersensitivity. When medications are injected 228, the insoluble particles, such as microcrystalline cellulose and talcum, become trapped in the pulmonary arterioles causing both thrombosis and inflammation. Over time, these particles can penetrate the arteriolar wall and provoke a giant cell granulomatous reaction. In animals, cotton fibres disrupt the PA wall, with further passage of the cotton fibres into the alveoli and interstitium 229. Within days after embolisation of cyano-acrylate, foci of medial and intimal necrosis have also been found in animal models 222. Confluence of the granulomas, subsequent fibrosis and distortion of the lung architecture, especially in the upper lobes, may occur. Pulmonary hypertension may develop as a result of chronic changes 230.
Birefringent material, such as that seen in talcum PE, is often but not exclusively demonstrated intracellularly in lung tissue (94%); this preferential pulmonary localisation is followed by the spleen, liver, lymph nodes and bone marrow. However, a granulomatous reaction was only observed in the lungs. Talcum was the only foreign material seen in organs other than the lungs, undoubtedly due to its smaller size 215. Intrapulmonary crospovidone embolism exhibits degenerative changes, contributing to vascular injury by causing angiothrombosis and granulomatous angiitis 216. In a consecutive series of 43 patients whose surgical lung biopsy demonstrated pulmonary infarction, embolotherapy and catheter embolism were observed in 2% of all cases 231.
Clinical signs
Most patients with talcum emboli are asymptomatic, although slowly progressive dyspnoea, persistent cough, nonspecific chest pain and occasionally anorexia, weight loss, fever and night sweats may occur. Lung sounds are usually normal or with minimal bibasal crepitations, and talcum deposits may be visualised in the retinal blood vessels 232. Clinical features appear to be dose-related and may progress even after drug injections have been stopped 2, 230. Multiple episodes of injection may thus elicit intractable pulmonary hypertension and death. Clinical symptoms associated with cellulose granulomatosis are also largely dependent on the extent of arteriolar involvement. Symptoms may range from none to exertional dyspnoea to sudden death 228. Two out of 47 children undergoing therapeutic embolisation of cerebral arteriovenous malformation developed severe respiratory distress that required endotracheal intubation 222. The clinical findings described in silicone embolism syndrome are very similar to those observed in FES. Dyspnoea, hypoxaemia, haemoptysis, alveolar haemorrhage, petechiae and altered consciousness were observed in a high percentage of these patients 221. A mortality of as high as 24% has been reported 221. Retained catheter fragments have been associated with an alarmingly high rate of complications 233: a 45–71% incidence of serious consequences 233, 234 such as arrhythmias, perforation, infection and thrombus formation were observed days to even weeks after embolisation. Embolisation of periprostatic seed implants after brachytherapy may be underestimated by the lack of induced symptoms 225 and they usually migrate after the day of implantation 235.
Diagnosis
Respiratory function tests generally show a persistent slight-to-moderate hypoxaemia and a reduction of carbon monoxide diffusion. Initially, imaging reveals several small (1-mm) nodular and reticular opacities or interstitial nodules, some of which occur in a centrilobular distribution throughout the lungs after talcum or cellulose granulomatosis 236. Later, homogeneous upper lobe opacities resembling massive fibrosis may be identified. Large pulmonary arteries and a large right heart may be observed in patients with pulmonary hypertension. Lymphadenopathy is rare 237. Gallium lung scans generally show diffuse bilateral uptake in talcum granulomatosis. BAL typically reveals lymphocytosis with a predominance of CD8 lymphocytes, and talcum crystals can occasionally be seen 238. Cellulose granulomatosis has also been described as a cause of the tree-in-bud appearance on high-resolution CT: micronodules distributed at the termination of bronchovascular bundles 160, 228. These micronodules represent intra-arteriolar accumulation of microcrystalline cellulose with adjacent granulomatous reaction. In mercury embolism, chest radiographic findings are striking: multiple small metallic spherules either distributed diffusely throughout the lungs or occasionally restricted to one or more dependent areas (fig. 4⇑). The opacities may be scattered or of different sizes or may appear as beaded chains simulating the appearance of an angiogram 220. The radiographic abnormalities may be permanent or may resolve gradually 220. In catheter emboli, radiographs may reveal a disconnected catheter fragment overlying an unexpected portion of the lung, mediastinum or heart. Generally, the course of the catheter corresponds to the expected location of the PA. Angiography or CT findings can obviously confirm the position of the catheter 2.
Definitive diagnosis requires histological examination of pulmonary tissue and is often only achieved at autopsy 212. With time, aspirated material is often incorporated into alveolar septae, at which stage it can be difficult to distinguish from organising microembolic intravascular material. A definitive diagnosis is obtained by examining transbronchial or open-lung biopsy specimens, which generally show macrophages with intracellular talc crystals. Microembolic foreign material generally elicits a granulomatous reaction 212. Identification of the particulates may require the use of ultrastructural analysis by analytical electron microscopy techniques, including selected area diffraction and X-ray energy-dispersive analysis 213. Polarisation microscopy is an ideal means of detecting foreign material such as intravascular deposits and aspirated foreign matter. Talc is distinguished readily by its appearance under polarised light: it exhibits a birefringent appearance with sharp, elongate fibres. Talcum does not stain with Periodic Acid Schiff (PAS), silver or Congo red 215. Cellulose particles are longer, mod-shaped, birefringent material 212. Crospovidone appears as basophilic, coral-like particles within arteries and extravascular granulomas 216. Organic starch has Maltese-cross morphology and stains positively with PAS 215. A collimated gamma scintillation survey meter may be used to detect iodine-125 seeds after prostate brachytherapy, as their small size means the seeds are frequently neglected on a radiograph 239.
Treatment
The prognosis for patients with mercury emboli is reported as good, although death has been reported 3. After several weeks, symptoms and functional impairments will diminish 240. Given the high complication rate associated with embolic catheter fragments, efforts should be made to recover foreign bodies prior to central embolisation 218. Many nonsurgical techniques have been developed to remove catheter material from the vessels, with a low complication rate 234. Talcum granulomatosis and embolisation of other foreign materials may develop into pulmonary hypertension and fibrosis. Treatment with corticosteroids has been attempted, with gradual or temporary improvement, although there is a risk of relapse after cessation 241. A number of patients with pulmonary disease due to injection of oral medications have undergone lung transplantation 242. However, recurrent and ongoing i.v. drug abuse, leading to a histiocytic reaction in the transplanted lung, should raise substantial concerns on performing lung transplantation in cases of substance abuse 242.
GAS EMBOLISM
The entry of gas into vessels was first described by Morgagni, whose post-mortem findings were published in 1769 243, 244. The first clinical report dates to 1821 244. Gas embolism (GE) is mainly air embolism (AE), although the use of other gases used in medical procedures or diving, such as carbon dioxide, nitrous oxide, nitrogen and helium, can also provoke these symptoms 245.
Incidence
The two different subtypes of GE, venous and arterial, can be distinguished by the mechanism of entry and the site where the emboli finally lodge. Preconditions for venous AE include a hydrostatic gradient favouring the intravascular entry of air and incising of noncollapsed veins: the epiploic and emissary veins, veins of the throat and dural venous sinuses in patients undergoing craniotomy in the sitting position 246. It may enter the veins of the myometrium 247 during surgical or diagnostic gynaecological procedures 248. The incidence of AE during surgery, as assessed by precordial Doppler, ranges from 7–69% 249.
Venous AE is often an iatrogenic problem during the manipulation of a central venous and haemodialysis catheter 250: the incidence ranges 1 in 47–3000, with a mortality rate even reaching 30% 251. It has been occasionally reported when a peripheral venous infusion was started 252 or after contrast-enhanced CT examination 253. The incidences during diagnostic cardiac catheterisation and percutaneous coronary intervention are 0.84% and 0.24%, respectively 254. AE is a rare complication of ventricular assist device pump dissection 255, ventilation-induced lung trauma 256 and laparoscopy which can lead to air, argon or carbon dioxide embolism 257, 258, Other causes include fibrinolytic pleural lavage 259, the intraoperative use of hydrogen peroxide, insufflation of air during endoscopy, laser therapy, arthroscopy, thoracotomy, noninvasive ventilation, carotid endarteriectomy or prostatectomy 245, 260.
The entry of gas into the pulmonary veins or the systemic arteries as a result of overexpansion of the lung by decompression barotrauma or a paradoxical embolism causes arterial embolism. Microbubbles, originating in extracorporeal devices but endogenous in cases of decompression sickness or mechanical heart valves, may cause arterial GE 261, 262.
Pathophysiology
Insidious venous AE causes a “string” of bubbles to enter the veins. Pulmonary vessel filtration protects the systemic and coronary circulation from AE orginating in the venous circulation 263. When air bubbles are finally trapped in the pulmonary capillaries, the pulmonary arterial pressure increases, and the increased resistance to right ventricular outflow diminishes pulmonary venous return resulting in diminished cardiac output 264. When >50 mL of gas is injected abruptly into human veins, acute cor pulmonale, asystoly or both can occur 265. The lethal volume of injected air in humans is estimated to range 100–500 mL 2.
The entry into the bloodstream requires a pressure gradient: when venous pressure is negative as during spontaneous inspiration, gas is forced under pressure 266; or when the vein is located higher than the heart 249. The alteration in the resistance of the lung vessels and the mismatch between ventilation and perfusion cause intrapulmonary right-to-left shunting and increased alveolar dead space leading to decreased gas exchange 267, arrhythmia 268, pulmonary hypertension 268, right ventricular strain 269 and arterial AE related to shunting 270.
Bubbles in vessels can be absorbed and adhere 271. Activated neutrophils sequestered in the pulmonary capillaries aggregate around the bubble 261. Prostaglandins are realised increasing permeability, causing lung oedema 272 and inactivation of surfactant with alveolar collapse and atelectasis 273. Impeded lymph flow by increased venous pressure further enhances lung oedema 274. AE during diving is the clinical manifestation of Boyle's law as the result of overdistention of the alveoli by expanding gases during ascent 244. A change in pressure of 70 mmHg, correlating with a full inspiration with compressed air at only 1 m under water, can cause barotrauma 275. Air bubbles entering via a catheter may even rise retrograde against the flow to the brain 276.
Arterial GE causes ischaemia. Two mechanisms for AE after lung surgery were historically recognised: infusion of air into the pulmonary vein and arterialisation of venous bubbles via a foramen ovale 277. Gas entry into the aorta obviously distributes bubbles into many organs. Small emboli in the vessels of skeletal muscles or viscera are tolerated, but hypoxaemia caused by obstruction of the coronary or cerebral arteries (cerebral arterial gas embolism (CAE)) may lead to fatality 245. Intracoronary injection of a bolus of air leads to depression of heart function 278. When bubbles occlude the brain vasculature, intracranial pressure (ICP) increases and ischaemia occurs 279. Microbubbles “irritate” the cerebral vascular wall, leading to a breakdown of the blood–brain barrier 280. Such tiny bubbles may briefly interrupt cerebral arteriolar flow 281. Normalisation is often only temporary, and blood flow may subsequently decrease to levels below those required to maintain neuronal function 282. Additionally, the contact of bubbles with the endothelium leads to activation of leukocytes in the damaged brain area 283. The coagulation system, complement and kinines, are activated by bubbles 284 but coagulopathies, common in animal models, are rarely observed in humans 244.
A paradoxical embolism occurs when gas in the veins manages to enter the systemic arterial circulation. This may be caused by passage across a patent foramen ovale, rendering right-to-left shunting of gas bubbles feasible 285. Elevated pulmonary arterial pressure due to venous GE may also result in elevated right atrial pressure, making it possible for a bubble to be transported through a patent foramen. Moreover, the decrease in left atrial pressure caused by ventilation, and the use of positive end-expiratory pressure may create a pressure gradient 265. Venous gas may also enter the arterial circulation by overwhelming the mechanisms that prevent arterial AE. This explains why CAE caused by a venous gas embolus has been described, although no intracardiac defects could be demonstrated 286. Various volatile anaesthetic agents diminish the ability of the pulmonary circulation to filter out gas 287.
Clinical signs
In venous GE, manifestations include cough, dyspnoea, tachypnoea and a hypoxaemic “gasp” reflex when 10% of the pulmonary vessels are occluded 249, 266. Arterial embolisation into the coronary arteries induces a specific drum-like or “mill-wheel” murmur and electrocardiographic changes of ischaemia 2. Arrhythmias, cardiac failure and arrest are all possible 288. Circulatory responses may also develop suddenly with embolisation to cerebral vessels 268. The absolute quantity of gas and the areas of the brain that are affected determine the variety of symptoms: haemiparesis, paresthesias, paralysis, seizures, visual disturbances and headache 244, 289. About 50% of patients will also have some history of (transitional) impaired unconsciousness 290. Asymmetry of the pupils, haemianopsia and impairment of the respiratory and circulatory centres (manifested as Cheyne–Stokes breathing) 268, 288 are other well-known complications. A delayed recovery from general anaesthesia may help detect CAE. Detection of air in retinal vessels and the occurrence of sharply-defined areas of pallor on the tongue have been described. Marbling of the skin may occur and is especially noted in superiorly located body parts because the distribution of air is determined by the principle of air buoyancy 264.
Diagnosis
The real diagnostic criterion is the patient's history. In venous embolism, the mill-wheel murmur, a splashing auscultatory sound caused by the presence of gas in the cardiac chambers and great vessels, can be auscultated. Chest radiograph findings include normal findings, radiolucency in the PA, heart and hepatic veins, pulmonary oedema, enlarged central pulmonary arteries, dilatation of the superior vena cava and atelectasis 2. Air in the distal PA may appear in a bell shape, and CT may reveal air in the veins, right heart or PA (fig. 6⇓) 2. A decrease in end-tidal carbon dioxide (ETCO2) levels, as determined by capnometry 291, suggests a change in the relationship between ventilation and perfusion. ETCO2 is the intraoperative standard and the magnitude and duration of ETCO2 decrease correlate with the volume of embolised air 249. Arterial saturation as measured by pulse oximetry is not able to detect AE as readily 292. Precordial Doppler ultrasonography is a sensitive means of detecting intracardiac air, often used during surgical procedures 249, 293. An even more sensitive method is echocardiography, which may detect air bubbles as small as 5 μm as white reflections and a patent foramen ovale 246. Intracardiac transvenous echocardiography was superior to other techniques for detecting venous embolism in a swine model 294. Gas bubbles in the retinal vessels can be identified. Another finding is haemoconcentration, possibly as a consequence of the extravascular shift of fluid into injured tissues 295.

Incidentally found air-emboli on cardiac computed tomography (CT) in an asymptomatic 62-yr-old male. Axial contrast-enhanced CT image shows multiple small air bubbles in the main pulmonary artery (arrows).
CAE can sometimes be seen on CT 296 but in divers with neurological symptoms, CT was unable to show any evidence of CAE 297. Abnormalities on brain MRI may range from no abnormalities up to local oedema, caused by an increased volume of water or hyperintense acute infarctions on diffusion weighted images 298. As no imaging technique alone has sufficient accuracy to warrant its use for diagnostic purposes, diagnosis should be made on clinical suspicion without reliance on imaging 244.
Treatment
Aggressive treatment is essential. For venous GE, the mainstays of treatment are the prevention of further entry of gas, volume expansion, administration of 100% oxygen and cardiopulmonary resuscitation, if necessary. The patient should be placed in the left lateral decubitus position to prevent right ventricular outflow obstruction by airlock 251. In a somnolent patient, resuscitation and intubation should be performed to maintain oxygenation 290. Bilateral manual jugular venous compression can elevate the cerebral venous pressure for embolism during intracranial procedures 299. Administration of up to 100% oxygen can decrease bubble size by establishing a diffusion gradient that favours the elimination of gas from the bubbles and by increasing the gradient for the egress of nitrogen from the bubbles 245, 300. Attempting to evacuate air from the right ventricle with the use of a multi-orifice central venous or pulmonary arterial catheter is recommended. Occasionally removal of up to 50% of the entrained gas can be achieved, with optimal placement of the catheter tip 2 cm below the junction of the superior vena cava and the right atrium 251, 265, 301.
Patients with arterial GE should be placed in the flat supine position. The buoyancy of gas bubbles is not sufficient to counteract blood flow, propelling such bubbles towards the head even when the patient is in a head-down position. In addition, the head-down position may aggravate cerebral oedema 302. A short period of hypertension that occurs following bubble lodging in the cerebral circulation is therapeutic because it facilitates bubble redistribution to the capillaries and veins 268. The treatment goal is to maintain at least normal blood pressure and to prevent hypotension 245. Seizures should be suppressed with barbiturates 289, thereby reducing cerebral oxygen consumption 303. For arterial GE, hyperbaric oxygen (HBO) is the treatment of choice as soon as stabilisation has been achieved. The patient breathes 100% oxygen at a pressure above that of the atmosphere at sea level, decreasing the size of the gas bubbles by increasing the ambient pressure. The hyperoxia produces diffusion gradients for oxygen into and for nitrogen out of the bubble 302. HBO decreases cerebral oedema, allows better oxygenation of already ischaemic tissue and diminishes the activation of leukocytes 289, 304, 305. Although recovery rates vary widely, early application of HBO plays an important role in the management of CAE: a significantly better outcome in patients with venous AE with a delay in treatment of less than 6 hours was reported 290. However, delayed treatment (up to 48 hours) may still ameliorate the patient's condition 306, 307.
As haemoconcentration leads to an increase in blood viscosity 295, 308, normovolemia should be achieved to optimise the microcirculation and to reduce neurological damage 309. Colloid solutions are preferable because crystalloid solutions may promote cerebral oedema. The use of corticosteroids in patients with arterial GE is even more controversial. CAE induces swelling of cells (“cytotoxic oedema”) 310, a type of ischaemic injury aggravated by corticosteroids 311. Animal studies suggest that lidocaine may be beneficial by preserving cerebral blood flow 244 and reducing ICP 245. In one clinical trial, lidocaine provided cerebral protection during cardiac surgery 312. The intravenous administration of fluorocarbons, characterised by high gas-dissolving capacity and low viscosity 313, should increase tissue oxygen delivery and shrink gas bubbles because of higher diffusion gradient. Animal studies demonstrated an improvement in cardiovascular function after AE 244, but more studies are needed to prove their efficacy in humans 314. Nitric oxide (NO) might be involved in the prevention of bubble formation, the central goal in decompression procedures. The intake of an NO donor reduces bubble formation following decompression in divers 315.
CONCLUSION
Adipocytes, as well as haematopoietic, amniotic, trophoblastic or tumour cells, can embolise to the lung. This list may be extended to bacteria, fungi, foreign material and gas. This diversity of emboli causes a wide variety of clinical signs also related to a complex and diverse pathogenesis. Far more complex than the “simple” mechanical obstruction after embolisation of vascular thrombi, nonthrombotic emboli may additionally lead to severe inflammatory reactions both in the systemic and the pulmonary circulation (fig. 7⇓). NTPE presents a formidable diagnostic challenge because the condition often presents with very unusual and peculiar clinical signs that are frequently overlooked. They range from very dramatic hyperacute presentations, such as ARDS in fat and AE, or signs observed late in the disease course, such as in tumour emboli. Pathological observations play a key role in the exact diagnosis, as sometimes carefully aspirated blood from the PA or specific staining of cells recovered from BAL fluid may be helpful in the diagnosis. Frequently, lung biopsies revealing the severe granulomatous reaction or unfortunate post-mortem pathological investigations of pulmonary tissue are necessary to confirm the diagnosis. On thin-section CT of the lungs, peculiar radiographic findings such a feeding vessel, the tree-in-bud pattern or the appearance of micronodules distributed at the termination of bronchovascular bundles may be seen in certain forms. From this review, we also hope to increase the awareness of acute and chronic NTPE as an underestimated cause of acute and chronic pulmonary hypertension. Despite the detailed descriptions of several forms of NTPE available for almost 100 years, well-designed trials have never been performed to evaluate therapy in the different subsets of these patients.

Different cell types (adipocyte, haematopoietic, amniotic, trophoblastic or tumour), bacteria, fungi, foreign material and gas may be carried in the blood stream and embolise to the pulmonary circulation. The complex and diverse pathogenesis of different subtypes of emboli is subject to continuing speculation and is certainly far more complex than “simple” mechanical obstruction after embolisation of vascular thrombi. Nonthrombotic emboli may also lead to a severe inflammatory reaction both in the systemic and pulmonary circulation, as well as in the lung. Acute and chronic nonthrombotic pulmonary embolism are an underestimated cause of acute and chronic pulmonary hypertension.
Statement of interest
None declared.
Acknowledgments
The secretarial assistance of V. D'Hoey and H. Fleurackers (Antwerp University Hospital, University of Antwerp, Belgium) is gratefully acknowledged. The artwork of figures 1 and 3 was designed by D. De Weerdt (DDW design, Edegem, Belgium).
- Received September 15, 2008.
- Accepted November 18, 2008.
- © ERS Journals Ltd
References
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵











{kind=link}
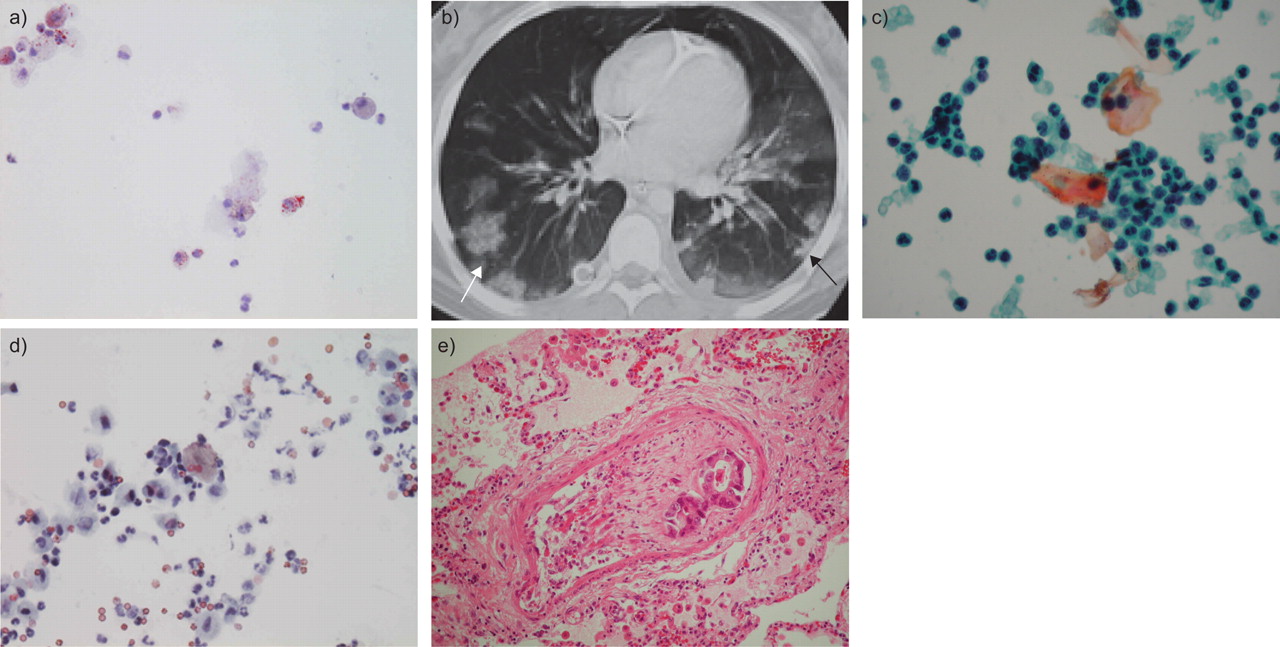{kind=link}
{kind=link}
{kind=link}
{kind=link}
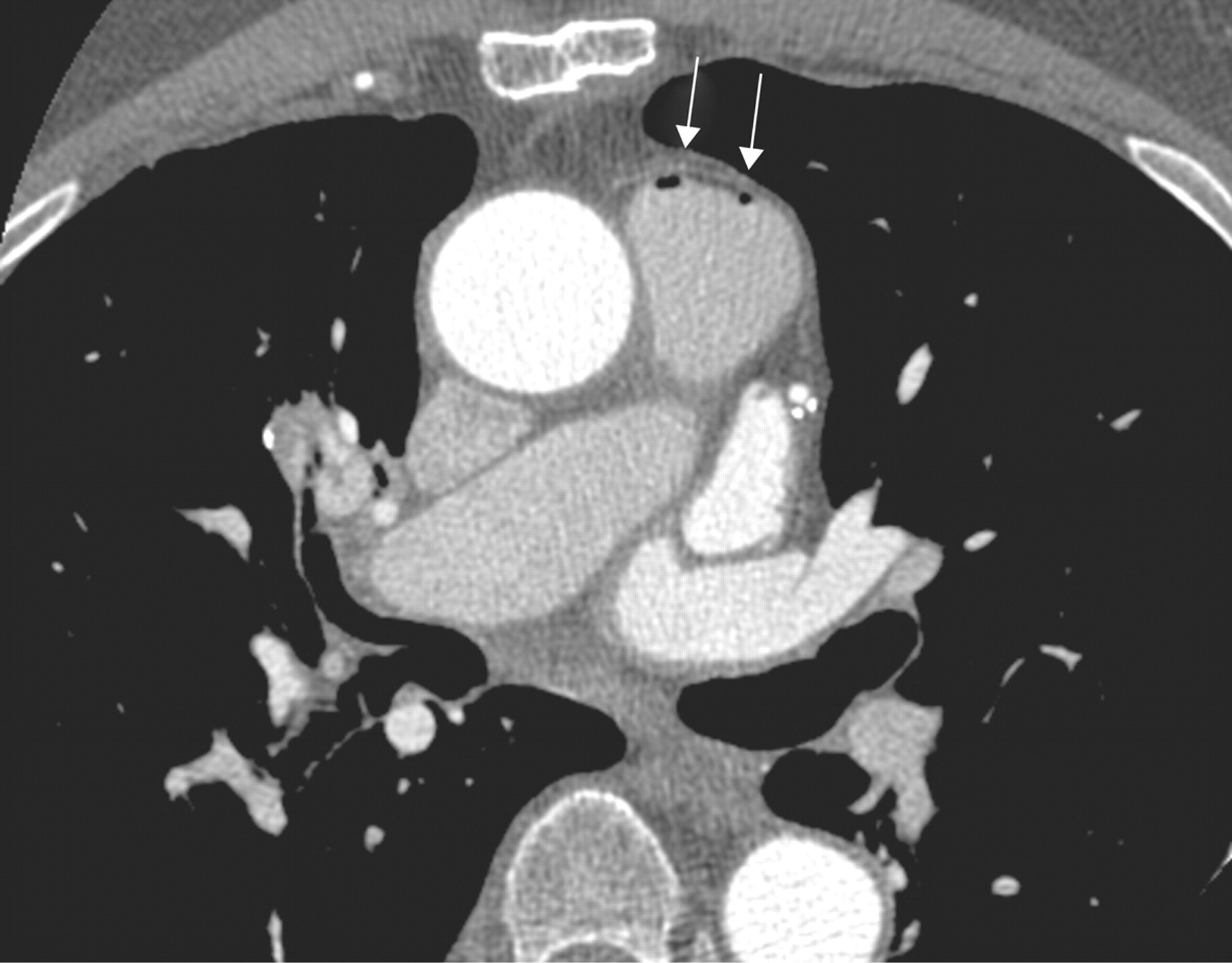{kind=link}
{kind=link}