
Abstract
The effect of various formulation and process parameters on the extraction of silicone from siliconized cyclic olefin copolymer (COC) syringes is reported. The impact of proprietary silicone curing process on COC syringe barrels was evaluated with respect to the rate and extent of silicone extraction. Similarly, the impact of formulation parameters such as pH, ionic species, and cosolvents on silicone extraction was also evaluated. The rate and extent of silicone extraction into contact solutions was inversely related to the degree of completion of the silicone curing process. The rate and extent of silicone extraction in solution were highest upon exposure to extreme pH solutions. The silicone extraction data indicate that the silicone curing process and formulation parameters have a profound effect on the rate and extent of silicone extraction into solutions.
LAY ABSTRACT: Silicone oils are used in medical syringes to provide lubrication. Prefilled medical syringes contain solutions into which silicone oil components may migrate. This study examined the degree to which silicone components migrated into different solution matrices. The impact of different levels of proprietary silicone curing processes on the migration of silicone components in contact solutions was also examined. This study also examined the impact of various formulation parameters (pHionic strength and cosolvents) on the degree to which silicone components migrated into solutions. Solution pH had the greatest effect on silicone migration with higher levels of silicone measured in solutions at the pH extremes. Curing of the silicone (reaction of the silicone with the syringe materials) also had significant impact. High curing levels resulted in less silicone migrating into solution as compared to levels seen with syringes with low curing levels. Thus it was demonstrated that both the nature of the solution stored in the syringe and the degree of silicone curing on the syringe barrel had substantial impact on the amount of silicone that migrated from the syringe components into the solution contained within the syringe.
Introduction
Cyclic olefin copolymer (COC) syringe barrels provide several advantages for prefilled applications. These advantages include clarity, inertness, light weight, and break resistance. COC syringe barrels are lubricated with silicone to improve functional properties such as piston breakaway and operational force. The properties that make silicone appropriate for lubrication include hydrophobicity and low glass transition temperature (1). Unfortunately, leachable silicone has been implicated in drug instability (2–7). Middaugh et al. (3) have shown that in the presence of silicone oil, various model proteins exhibited a higher propensity to aggregate. Markovic (2) reported that the incompatibility of silicone with a drug product led to particulate formation.
Silicone oil can simply be applied on syringe barrels by spraying techniques. The sprayed silicone can undergo further process of baking on syringe barrels. Alternatively, the silicone oil can also be applied by a curing process on syringe barrels. The impact of variations in a proprietary silicone curing process with COC syringe barrels was evaluated with respect to the amount of silicone extraction into contact solution. This paper also presents a systematic evaluation of various formulation parameters on the rate and extent of silicone extraction into contact solution upon storage in COC syringes. Formulation parameters such as pH (2–12), presence of cosolvents (alcohol), and ionic species were assessed. The purpose of the evaluations was to determine the suitability of siliconized COC syringe barrels for various types of injectable formulations with respect to silicone leaching into drug solution.
Test Article Preparations
COC syringes with elastomeric tip caps were filled with various contact solutions (Tables I and II) and manually closed with elastomeric pistons. Filled syringes were stored in controlled temperature chambers (5 °C, 25 °C, 40 °C, or 55 °C) for as long as 12 weeks. Syringe contents were brought to ambient temperature before testing. In addition, the solution from the extracted syringes was concentrated using solvent extraction.
Formulation Recipes of Various pH
Additional Formulation Preparations at pH 2.3
Methodology
Solutions from siliconized and nonsiliconized syringes stored at refrigerated and accelerated temperatures for up to 12 weeks were analyzed by inductively coupled plasma–atomic emission spectroscopy (ICP-AES), total organic carbon (TOC), and gas chromatography–mass spectrometry (GC/MS) to determine the extent of silicone extraction from the syringe barrels. The silicone in solution was measured by ICP-AES as elemental silicon. The TOC analysis determined the total amount of extractable carbon in various solutions, and the GC/MS identified the types of silicone and other organic extractables responsible for the TOC and Si in the solutions.
Silicon Detection by Inductively Coupled Plasma–Atomic Emission Spectroscopy (ICP-AES)
The test solutions from syringes were extracted with methyl isobutyl ketone (MIBK) in a separatory funnel. The aqueous layer was separated and analyzed for silicon using elemental silicon standard.
Total Extractable Content Determined by Total Organic Carbon (TOC)
An OI Analytical Model 1010 TOC analyzer was used for all TOC measurements.
Results/Discussion
1) Determination of Silicone Extractables in Various Formulation Types Stored in COC Syringes
1A) Determination of Silicone Extractables across a Broad pH Range (pH 2–12):
Silicone-related extractables (quantified as silicon using ICP-AES calibrated with elemental silicon) were measured in siliconized and nonsiliconized (control) COC syringe solution contents spanning a broad pH range (pH 2–12). Both the control and siliconized syringes contained elastomeric silicone components. Silicone levels measured in solutions stored in the control syringes were low (<0.2 ppm) for all solutions studied at all time points, indicating that the contribution of silicone extracted from the elastomeric components was low. The silicon results for the solutions stored in siliconized syringes are displayed in Figure 1.
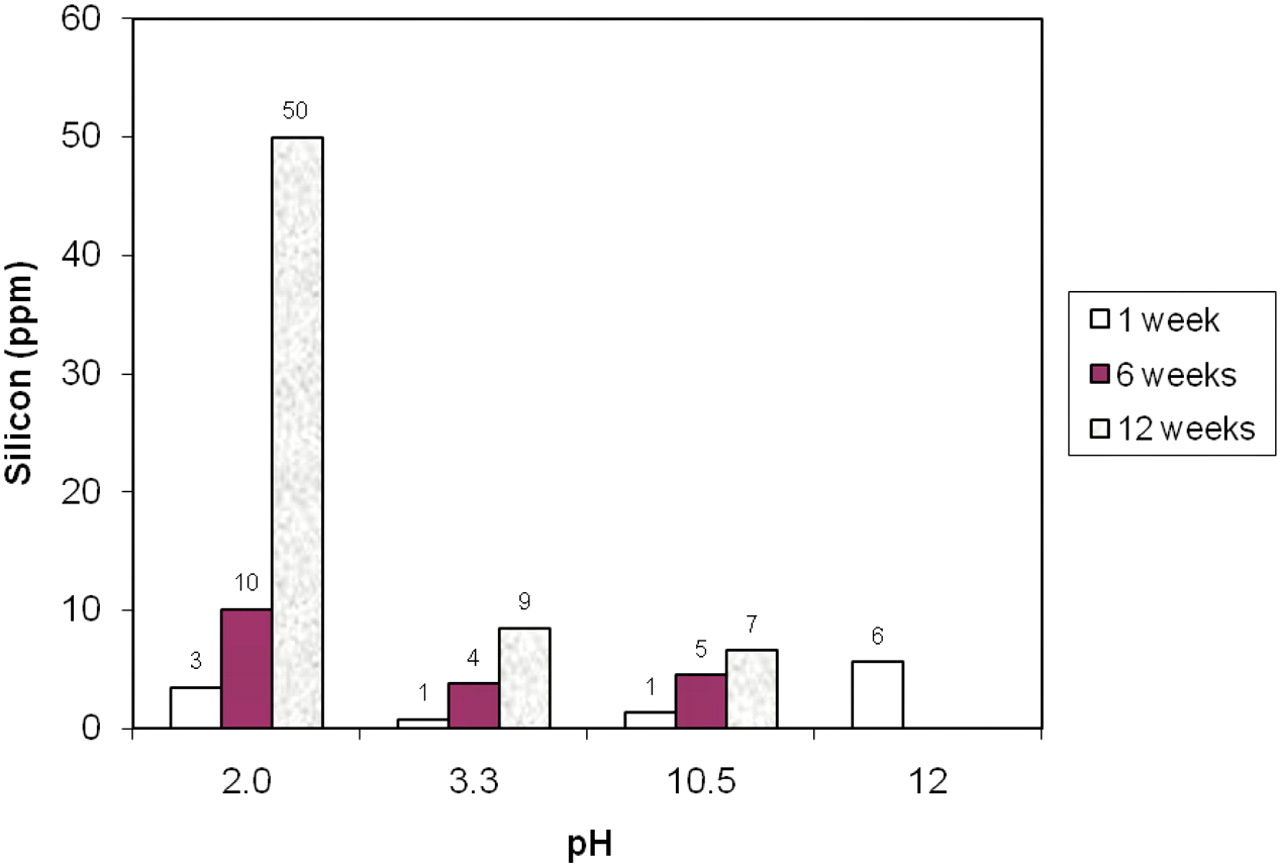
Effect of pH on silicone extraction (measured as silicon) upon storage at 55 °C (siliconized COC syringe, COC syringe lot #1). Data of the pH 12 solution were limited to one week at 55 °C storage condition because testing of pH 12 test articles was discontinued after one week storage.
Data for the pH 12 solution syringes was limited to 1 week at a 55 °C storage condition because testing of pH 12 test articles was discontinued after 1 week of storage. Extractable silicone levels in solutions from siliconized syringes were observed to be significantly higher at pH 2 than at pH 3.3 and pH 10.5. Although limited silicone extractable data were generated for pH 12 solutions relative to the other pH solutions (conducted at 1, 6, and 12 weeks, as listed in Figure 1), the pH 12 solution data indicate that the rate and extent of silicone extraction was comparable to pH 2 solutions and greater than in the pH 3.3 and pH 10.5 solutions. The conclusion that elevated silicon extractable levels are observed in pH 12 solutions stored at accelerated temperatures (55 °C) is strengthened further upon observing similarly elevated silicone levels during the narrow pH range (pH 10–12) testing shown in Figure 2. The levels of extractable silicone in pH 3.3 and pH 10.5 contact solutions were similar and lower than in the pH 2 and pH 12 solutions. These solutions contained different salts (citrate/NaCl vs phosphate), but were prepared at the same tonicity (Table I).
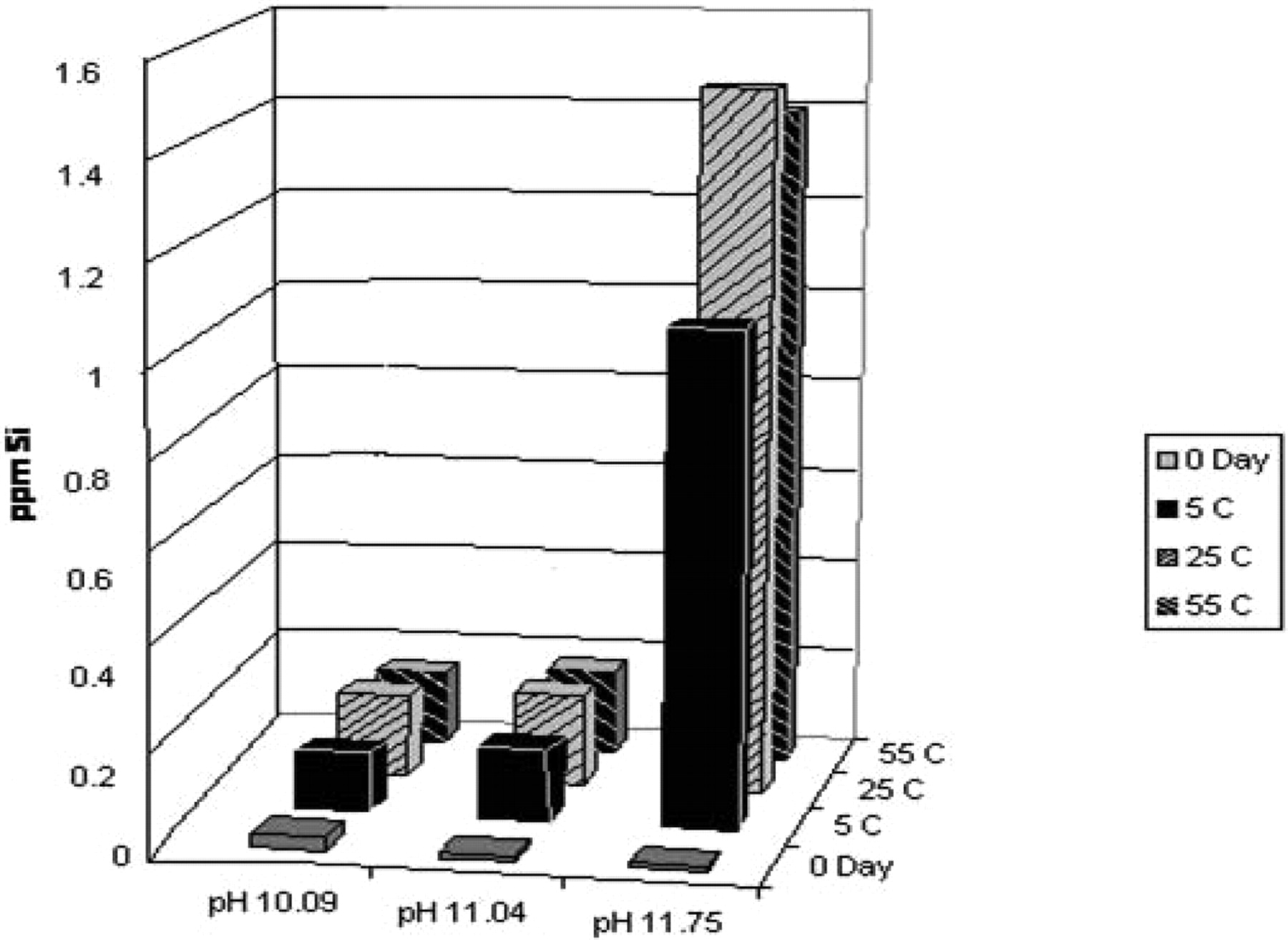
Silicon accumulation over narrow basic pH range (pH 10–12).
Silicone-related extractables (as silicon) and TOC were measured for pH 2 (prepared with HCl) and pH 10 contact solutions after 3 and 6 months of storage at 25 °C and 40 °C. Results for both silicon and TOC appear in Table IV. At extreme pH, the silicone-related extractables become the primary extractable species. This was demonstrated by high silicon/TOC % reconciliation values observed in pH 2 solutions stored in COC syringes. The silicon/TOC percentage reconciliation was lower for the pH 10 solution and was demonstrated to be due to the presence of other extractables, such as fatty acids that originated from elastomeric components.
Silicon TOC Reconciliation
1B) Silicone Extractable Determination across Narrow pH Ranges (pH 10–12):
The observation of high silicone extractables levels upon exposure of COC syringes to high pH solutions was examined in more detail with contact solutions prepared at pH 10.1, pH 11.0, and pH 11.75 (pH ∼12). The syringes were stored at 5 °C, 25 °C, and 55 °C for 4 days. The extractable silicon levels after 4 days of storage are shown in Figure 2. Accumulation of silicone was higher in the pH 11.75 solutions stored in siliconized COC syringes (greater than 1 ppm) as compared to the same syringes filled with pH 10 and pH 11 solutions (less than 0.2 ppm).
1C) Silicone Extractable Determination across Narrow Acidic pH Range (pH 2–3):
The observation of high levels of silicone extractable upon exposure of COC syringes to low pH solutions was examined in more detail with contact solutions prepared at pH 2.0, pH 2.3, and pH 3.0. The results presented in Figure 3 illustrate the dependence of the accumulation of silicone in solution on the pH of the solution. These low pH solutions had the same constituents at similar concentrations to give similar tonicities. All solutions were highly hypotonic. The silicone accumulation after 6 weeks of storage was highest at pH 2.0 (30 ppm) and significantly reduced at pH 3.0 (4.4 ppm).

Effect of various low pH solutions on the rate and extent of silicon extraction into contact solutions (siliconized COC Syringe, 55 °C storage, COC syringe lot #2).
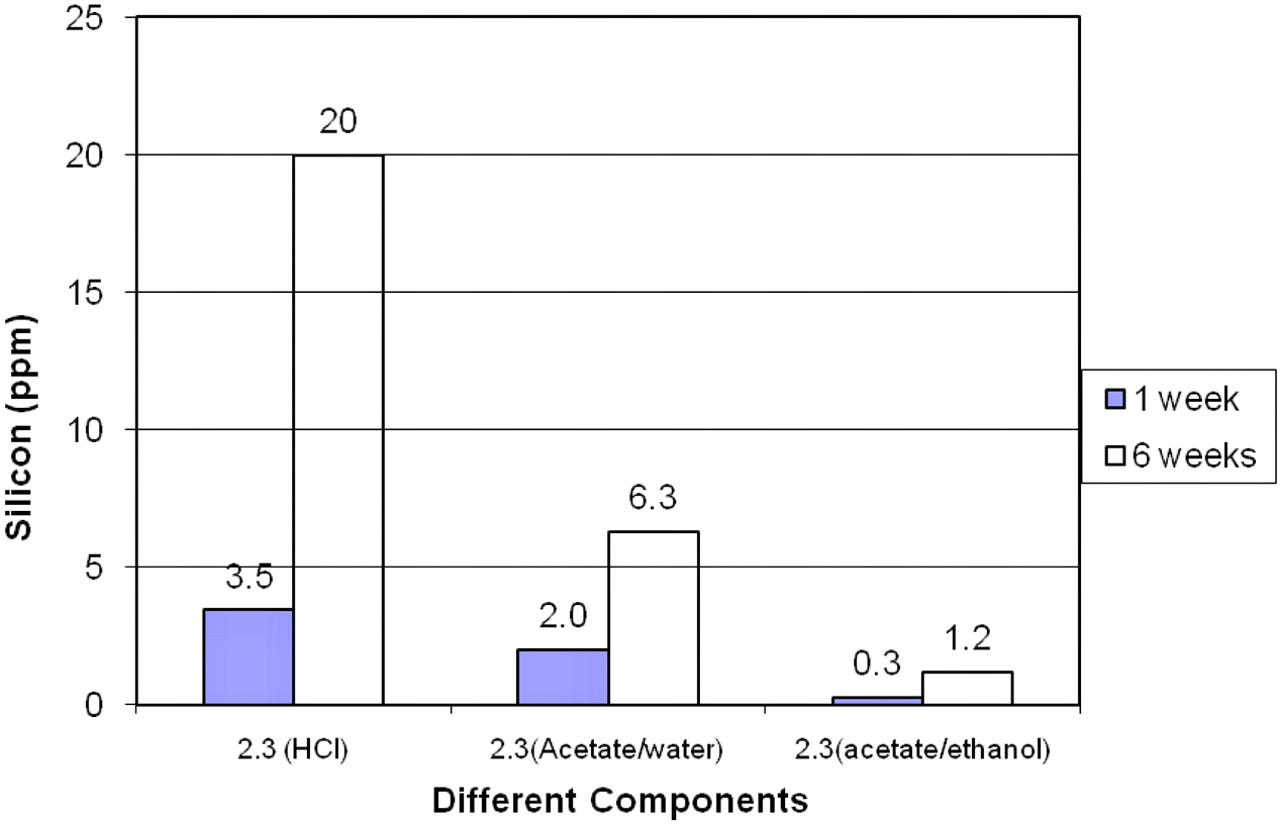
1D) Silicone Extractable Determination in Various pH 2.3 Solutions:
Acidic pH 2.3 solutions of 10 mM KCl (containing HCl), 0.6 N acetic acid, and 0.6 N acetic acid in 40% ethanol were used to extract silicone from siliconized COC syringes (Table III). Levels of extractable silicone were lower in the acetic acid contact solutions than the KCl/HCl solution after storage at 55 °C for 1 or 6 weeks. Extractable silicone levels were the lowest in the ethanolic acetic acid solutions. The data, presented in Figure 4, indicate that the rate and extent of silicone extraction into various contact solutions at the same apparent pH (pH 2.3) was dependent upon the ionic species in solution. Contact solutions prepared with acetic acid showed significantly fewer silicone-related extractables than those solutions prepared with HCl, although both solutions were titrated to pH 2.3. Furthermore, contact solutions prepared with acetic acid in ethanol (40%) instead of water contained even lower levels of silicone-related extractables after accelerated storage in the COC syringe. The observation of lower silicon levels in the pH 2.3 acetate solution containing 40% ethanol than the same solution in the absence of ethanol may be attributable to a different mechanism of silicone degradation, related to solution polarity or the difference in hydrogen ion concentrations, despite the same apparent pH for these solutions.
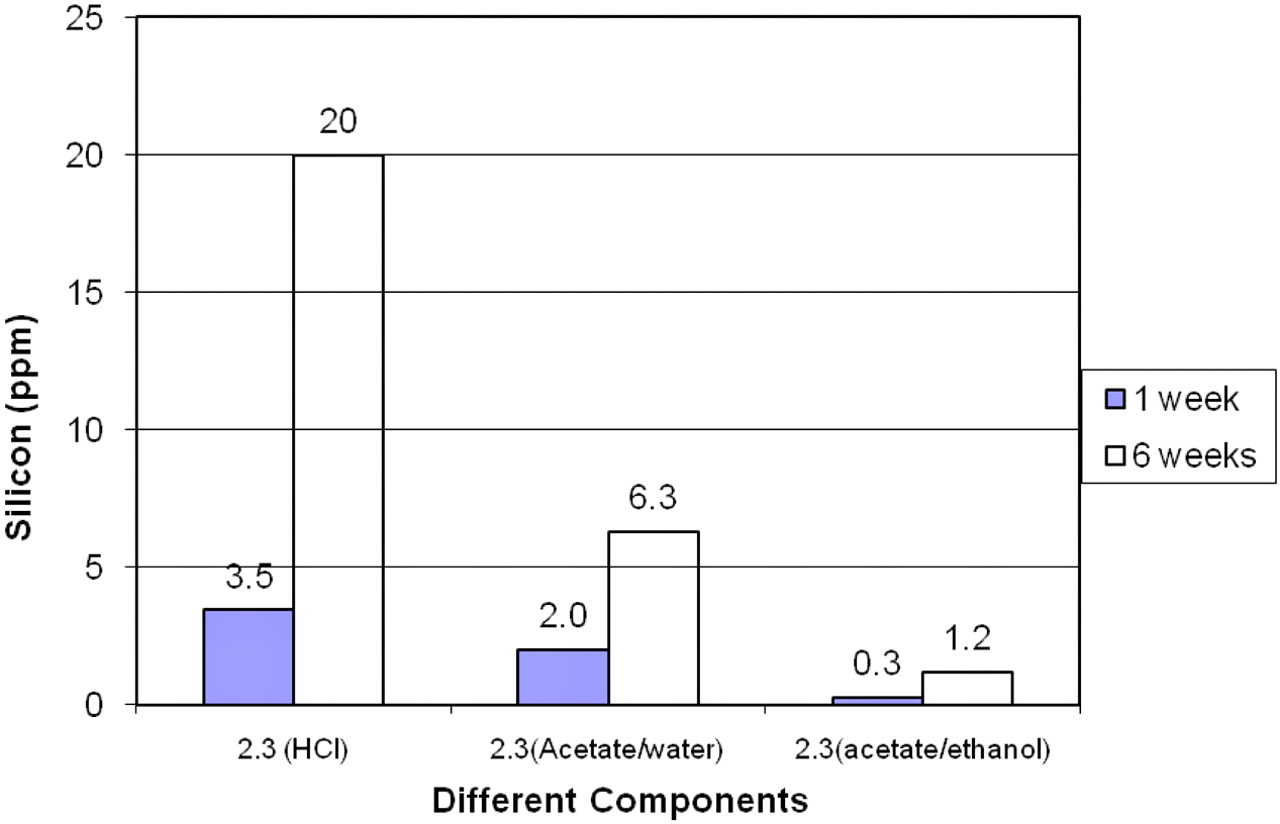
Effect of different contact solutions at same apparent pH upon silicon extraction (Siliconized COC syringe, 55 °C storage, COC syringe lot #2).
2) Identification of Silicone Extractables in Extreme pH Solutions
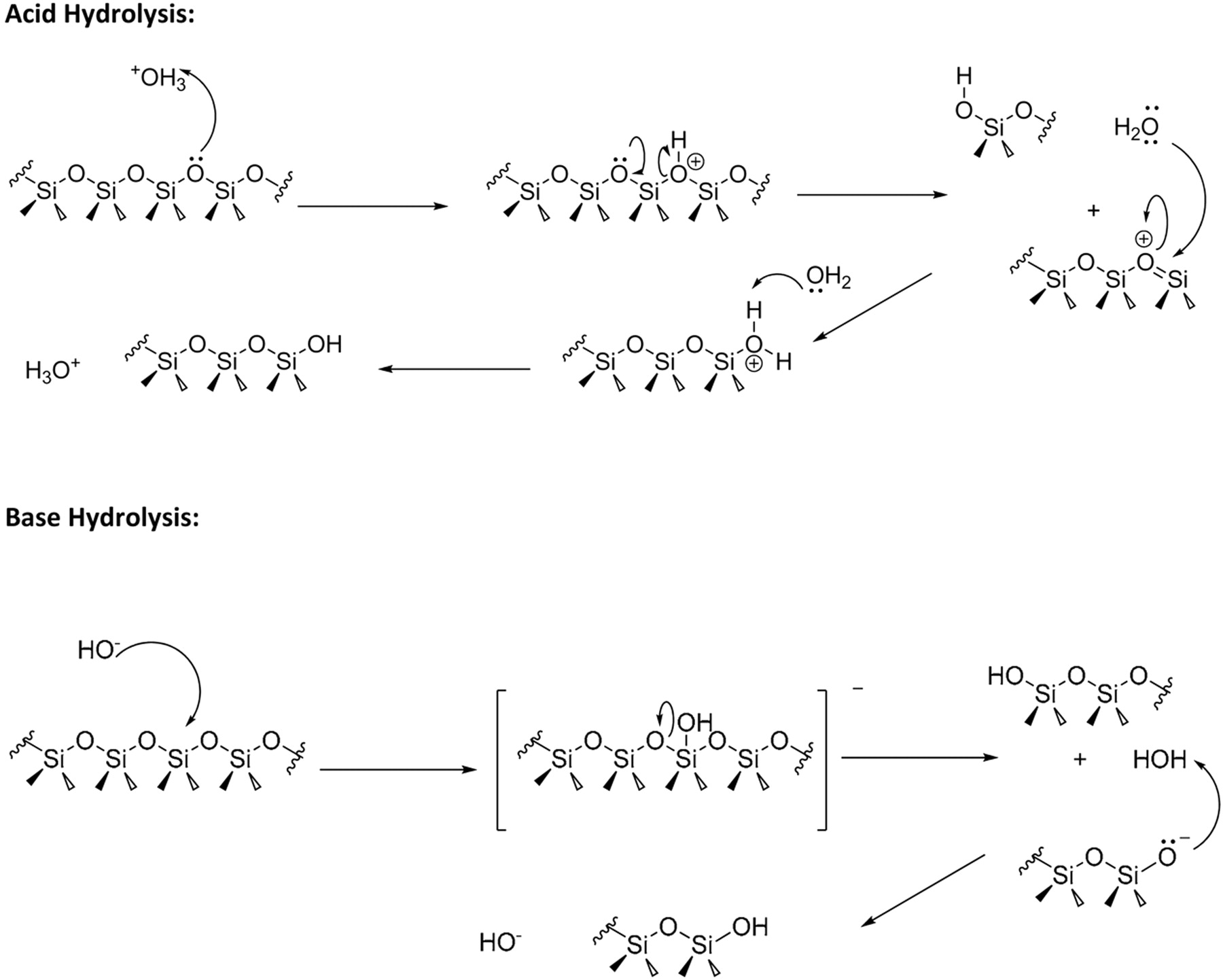
The pH 2 (prepared with HCl) and pH 12 contact solutions in COC syringes were examined by GC-MS to establish the structure of the silicone-related compounds present. The primary compounds responsible for the elevated silicon levels were found to be dimethylsilanediol and oligomers of dimethylsilanediol. Extreme pH contact solutions contained primarily dimethylsilanediol with lesser amounts of higher oligomers. GC-MS with cool on-column injection was used to verify that these compounds exist primarily as open-chain diols in solution. Small amounts of cyclic dimethylsiloxane components were also observed in these injections. Both extreme pH solutions (pH 2 and pH 12) had similar profiles when analyzed under acidic conditions. Silicone-related extractables, therefore, exist primarily as linear diols in solution. These compounds are consistent with the hydrolysis of the polydimethylsiloxane compound (Figure 5). Silanols are intermediates in every hydrolysis reaction of a silicone-functional group; however, they are not often isolated (9). Traces of acid or base catalyze their condensation to siloxanes and water.

Mechanism of degradation of silicone in extreme pH conditions.
3) Determination of the Effect of Silicone Curing on Silicone Extractables
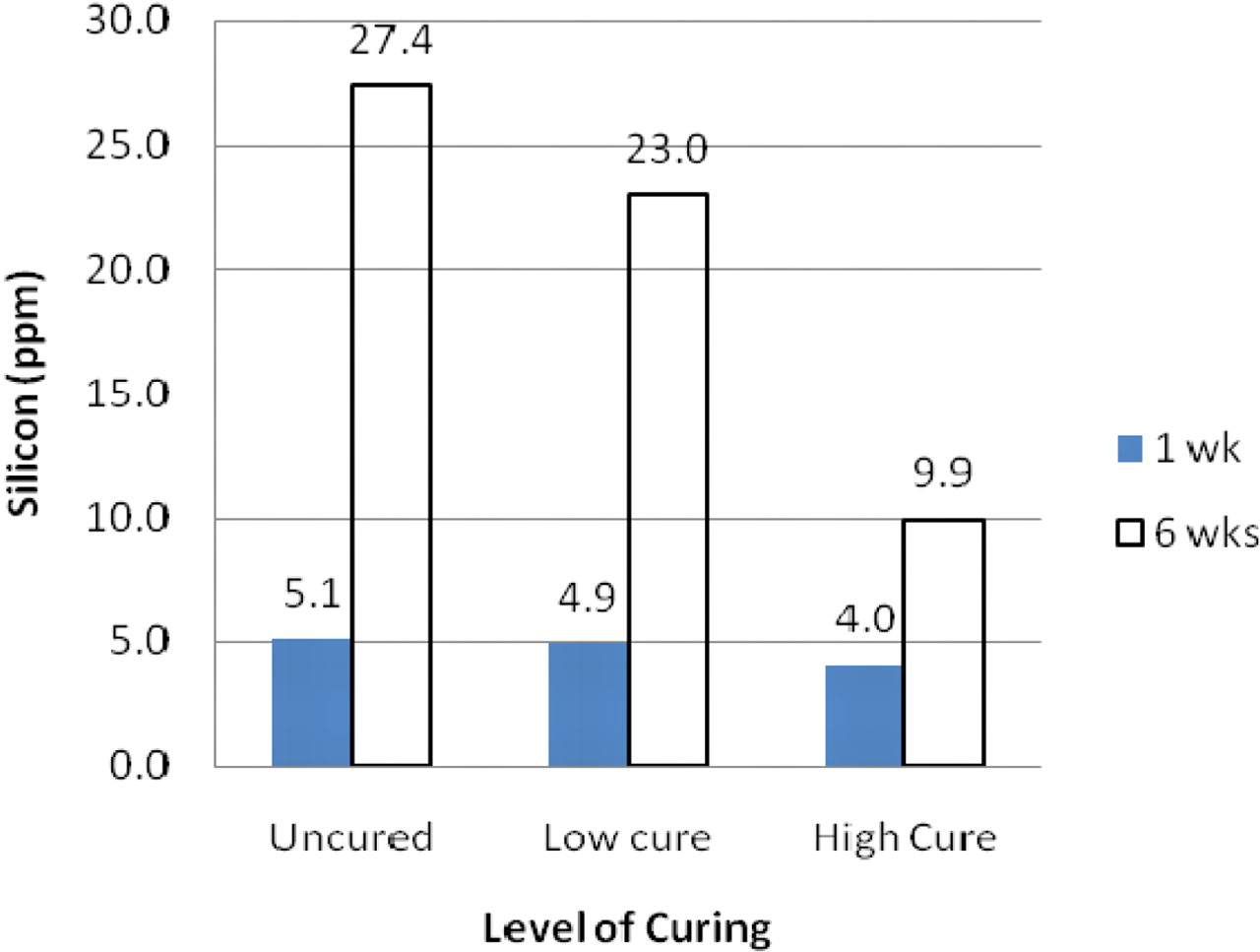
Using pH 2 (HCl) contact solutions, COC syringes with two levels of curing and one uncured were compared for silicone extractables. Measured silicon levels are shown in Figure 6. A higher accumulation of silicone-related extractables was observed in uncured and low-cured COC samples relative to highly cured COC samples after storage at 55 °C for up to 6 weeks. This is consistent with a decreased degradation rate of the silicone and could be attributed to decreased accessibility of the contact solution to cleavage sites within the silicone polymer and/or reduced solubility of the higher molecular weight silicone that was observed in cured syringes.

Effect of curing on silicon extractable upon storage with pH 2.0 solution at 55 °C.
Conclusions
Rapid hydrolysis of polydimethylsiloxane occurs in contact solutions of extreme pH (less than or equal to pH 2 and greater than or equal to pH 12) and is associated with increased silicone-related extractables in solution. The silicone extractable data further indicate that silicone processing parameters on COC syringe barrels such as curing as well as the formulation variables such as pH, ionic species, and/or cosolvents present the need to be considered for their impact on the rate and extent of silicone extraction from COC syringe barrels.
Conflict of Interest Declaration
There is no financial interest related to the manuscript.
Acknowledgments
The authors are grateful to Dr. Dennis Jenke and Martha Gill for their review of the manuscript.
- ©PDA, Inc. 2011




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}