
Abstract
The development of protein therapeutics requires stabilization of these labile molecules during shipment and storage. Biologics, particularly monoclonal antibodies, are frequently packaged at high concentration in prefillable syringes traditionally made of glass. However, some biologics are unstable in glass due to sensitivity to silicone oil, tungsten, glue, or metal ions. Syringes made from the plastic cyclic olefin polymer, Daikyo Crystal Zenith® (CZ), with a Flurotec-laminated piston, have none of these issues. This study compared the stability of several proteins including biotherapeutics when stored up to 14 months at 5 °C and 25 °C in prefillable siliconized syringes made of glass or silicone oil-free CZ syringes, and when subjected to mild agitation by end-over-end rotation at room temperature. At each time point, proteins were analyzed by several techniques including turbidity, size exclusion high-performance liquid chromatography, reversed phase high-performance liquid chromatography, ion-exchange chromatography, electrophoresis, and light scattering to monitor changes in aggregation and degradation. The results show that proteins have comparable stability when stored in glass syringes or in syringes made of CZ sterilized by E-beam or autoclave. In addition, proteins stressed by agitation were generally more stable and aggregated less in syringes made of CZ than in ones made of glass.
LAY ABSTRACT: Biotherapeutic protein drugs such as monoclonal antibodies are frequently packaged at high concentration in prefillable syringes, which allows the drug to be directly administered by the patient or caregiver. Protein drugs, or biologics, can be unstable, and may aggregate, particularly when shaken. These aggregates can be immunogenic, stimulating the body's immune system to produce antibodies that can reduce the drug's efficacy. Although prefillable syringes are traditionally made of glass, some biologics are unstable in glass syringes due to the presence of substances used in their manufacture, including silicone oil, which is necessary for lubricity. Syringes made from the plastic cyclic olefin polymer, Daikyo Crystal Zenith® (CZ), have none of these issues. This study compared the stability of several biotherapeutic proteins when stored up to 14 months at 5 °C and 25 °C in prefillable siliconized syringes made of glass or silicone oil-free CZ syringes, and when mildly agitated at room temperature. Proteins were analyzed by several techniques to detect changes in aggregation and degradation. The results show that biotherapeutic proteins have similar stability whether stored in syringes made of glass or CZ. In addition, proteins subjected to agitation were generally more stable and aggregated less in CZ syringes than in glass syringes.
- Prefillable syringe
- Silicone oil
- Tungsten
- Crystal Zenith
- CZ
- Protein aggregation
- Biotherapeutic protein
- Protein stability
Introduction
The last decade has seen a dramatic increase in the development and availability of biotherapeutic proteins to treat a variety of chronic diseases, particularly in the areas of oncology and autoimmune disorders. At the same time, the pharmaceutical industry has transitioned to using prefillable syringes both to package and deliver biotherapeutics. This has enabled more rapid and accurate dosing while improving patient compliance and safety, and reducing the cost associated with the additional drug product needed to overfill vials. Unlike small-molecule drugs, protein-based therapeutics, by their size, chemical reactivity, and amphiphilic nature, are more prone to degradation and aggregation. There is strong evidence that aggregated proteins, even those with native-like conformation, are capable of inducing an immunogenic response that could result in the production of neutralizing antibodies able to bind to and inactivate the drug, thereby reducing its efficacy (1⇓–3). In some extreme cases, if the biotherapeutic is a naturally occurring protein, such antibodies could endanger patient safety (2). However, others contend that the link between aggregates and clinical immunogenicity has not been unequivocally established; furthermore, they emphasize that subvisible particles are and have been present in products that have been on the market for years, and that these remain safe and efficacious (4).
Syringes made of glass have long been the industry standard for the delivery of injectable drugs. However, silicone oil, required for lubricity in glass syringes, has been shown to cause aggregation of some proteins including biotherapeutics (5, 6), and its interaction with proteins continues to be an area of active research. Moreover, silicone oil droplets from the barrel can interfere with quantification and characterization of protein particulates (7). Recently, Gerhardt et al. (8) proposed a model of particle generation in prefillable glass syringes in which proteins first adsorb to the hydrophobic surface created by the silicone oil to form a gel. In the presence of an air bubble that is capable of moving during handling and transport, capillary forces at the silicone oil–water–air contact line are sufficient to dislodge silicone oil and gelled protein aggregates from the interface and transport them into the bulk solution. This type of interfacial mechanism can explain the synergistic effects of silicone oil–water interfaces, air–water interfaces, and agitation in the generation of silicone oil–protein complexes in addition to silicone oil and pure protein aggregates observed in solutions stored in glass syringes.
Contaminants generated during the manufacture of glass syringes can also cause physical or chemical damage to proteins. The process of heating a tungsten wire to high temperature in order to form a hole for insertion of the needle can result in the deposition of various tungsten polyanionic species primarily in the funnel region of the syringe barrel (9), and this can cause some proteins to aggregate, particularly under acidic conditions (10, 11). In addition, acrylic acid capable of reacting with proteins can leach from adhesives used in glass syringes to fix the needle in place (12).
Over the last several decades, advances in the synthesis of plastics has led to the development of the class of cyclic olefin polymers (COPs) (13). These materials have high purity, as well as additional desirable properties including moldability and transparency. Syringes made from the COP Crystal Zenith® (CZ) do not require silicone oil for lubricity, and a tungsten pin is not used to form the opening for the needle because the needle is inserted during the molding process (14). In addition, unlike glass syringes, an adhesive is not employed in staked-needle syringes made of CZ. The performance of syringes made of CZ or similar materials with biologics has only recently begun to be evaluated. In one study, several model protein formulations were subjected to agitation in polymer-based (plastic) prefillable syringes. This investigation showed that higher levels of total subvisible particles and protein aggregates were generated in the siliconized plastic syringes than in a silicone oil–free system (15). The results suggest that in cases where a biotherapeutic has been shown to be prone to aggregation due to silicone oil, syringes made of plastic can provide a suitable alternative.
The current investigation was designed to compare the stability of proteins in glass versus CZ prefillable syringes and consists of three parts. Study I describes a method to analyze the tungsten and silicone oil content of prefillable syringes. This method was then applied to estimate the amount of both substances in the glass syringes used in this study as well as CZ syringes, which should not contain detectable levels of either material. Study II (a) compares the stability of several biotherapeutic proteins when stored in syringes made of glass or CZ for a period of about 1 year at 5 °C and under thermal stress at 25 °C, and (b) investigates whether sterilization of CZ syringes barrels by E-beam or autoclave affects protein stability. Study III examines the effect of mechanical stress produced by agitation on the aggregation of several proteins in both glass and CZ syringes.
Methods and Materials
Prefillable 1 mL long 27 G silicone oil–free Daikyo Crystal Zenith® (CZ) plastic and sterilized prefillable siliconized glass 1 mL long syringes were used. Syringe barrels made of CZ were sterilized by E-beam irradiation or autoclave. Plungers sterilized by autoclave were laminated with Flurotec,® a polymer film made from ethylene tetrafluoroethylene, to minimize the effect of potential leachables on protein stability. Luer lock 1 mL syringes were used in some agitation experiments to determine whether there were any significant differences between the two types of syringes on protein stability.
Chymotrypsinogen A and human Immunoglobulin G (IgG) were purchased from MP Biomedicals (Santa Ana, CA). Rabbit IgG was obtained from Rockland Immunochemicals (Pottstown, PA). Five protein drug products, A–E, were late-stage development commercial molecules not known to be silicone oil–sensitive. Abatacept, a silicone oil–sensitive biotherapeutic, was purchased as the lyophilized powder Orencia.® Prior to filling the syringes, the powder in the vial was reconstituted to a nominal concentration of 25 mg/mL with 10 mL of water using a silicone-free syringe provided by the manufacturer (16). All protein solutions were filtered through a 0.2 μm polyvinylidene difluoride (PVDF) syringe filter prior to use.
Deionized water equivalent to Milli-Q™ grade was used to prepare all buffer solutions, which were further filtered using 0.1 μm PVDF filter membranes (Millipore, Billerica, MA).
Study I—Tungsten and Silicone Content of Prefillable Syringes
Tungsten was analyzed using inductively coupled plasma mass spectrometry (ICP-MS) on a Perkin-Elmer/SCIEX Elan DRC II. Tungsten was extracted from glass or plastic syringes by drawing up 1 mL 2% HNO3 or 1 mL 5% NH4OH into each and sonicating the filled syringes for 1 h at 50 °C. The extracts were expelled, and the syringes were flushed with an additional 1 mL of solvent. The extract and the rinsate were pooled and brought to 3 mL with water. The lower limit of quantification is ∼2.5 ng/mL, corresponding to ∼8 ng/syringe.
Silicone was determined by atomic absorption spectroscopy on a Perkin Elmer AAnalyst 100. The needles were cut off four CZ 1 mL long syringes or four glass syringes (∼100 cm2 barrel surface area) as close to the barrel as possible. The syringes were extracted with 50 mL methyl isobutyl ketone to solubilize the silicone. The same volume of solvent served as a blank. The lower limit of quantification is ∼8 μg/mL, corresponding to 100 μg/syringe.
Study II—Long-Term Stability
Syringe fill and storage: The properties of the proteins used in long-term stability studies are listed in Table I. The syringes were filled with 0.5–1.0 mL protein solution using a Gilson Pipetman,® triplicates were prepared for each time point and temperature, and the pistons were vacuum-placed using an automated placement device. The syringes were placed tip down in a tub and stored under two conditions: in a refrigerator at 2–8 °C (referred to as “5 °C” throughout this study) and in a stability chamber maintained at 25 °C/60% relative humidity (RH); samples were removed for analysis at 1, 3, 6, 9, and 12, or 14 months. Solutions of each drug stored at 2–8 °C in borosilicate glass vials served as controls.
Properties of Biotherapeutic Proteins in Long-Term Stability Study
Study III—Protein Stability under Mechanical Stress
Syringe Agitation:
Agitation consisted of end-over-end rotation (7–10 rpm) on a rotating wheel at room temperature (RT) for periods of time up to 3 months. Proteins were diluted or dissolved to a final concentration of 1 mg/mL in 20 mM sodium phosphate/150 mM NaCl (pH 7.0) (PBS (7.0)) unless noted otherwise; concentrations were estimated spectrophotometrically using published extinction coefficients or ones calculated from the amino acid sequence. Syringes were filled with 1.1 mL of protein solution, and the height of the air bubble in each syringe was approximately 2 mm. All samples were run in triplicate. Table II summarizes the properties of the proteins used in this study.
Properties of Proteins in Stress Study
Measurements:
For each protein, the UV absorbance at 280 nm and the optical density at 350 nm was measured at the start of the experiment to determine protein concentration and to establish a baseline for the turbidity measurements. Samples of each protein were analyzed prior to filling the syringes and served as controls for each study. In the agitation experiments each type of syringe was also filled with protein solution and stored tip-down at 5 °C or at RT without agitation for the duration of the experiment. However, the absorbance of solutions stored at RT did not differ significantly from those stored at 5 °C or from the controls.
Analytical Methods:
Turbidity—Protein turbidity was measured at 350 nm on a Perkin-Elmer Lambda 35 UV/Vis spectrophotometer.
Chromatography—Chromatography was carried out on Waters Model 2695 liquid chromatography modules at RT unless otherwise noted. Proteins were detected at 214 and 280 nm. Waters Empower software was used to integrate chromatograms.
Size exclusion high-performance liquid chromatography (SE-HPLC)—Proteins were analyzed at RT on a GE Healthcare Superdex 200 or Sephadex G75 column (1 × 30 cm) after centrifugation to remove any insoluble material that could foul the column. This material was not further evaluated. Columns were equilibrated in 20 mM sodium phosphate/150 mM NaCl (pH 6.8) (PBS (6.8)).
Reversed phase high-performance liquid chromatography (RP-HPLC)—Proteins A, B, and D were analyzed on a Vydac C4 column (4.6 × 250 mm) at 60 °C. Protein C was chromatographed on a Vydac C4 column (2.1 × 50 mm). Columns were equilibrated in 0.1% trifluoroacetic acid in water, and proteins were eluted with a gradient of acetonitrile in 0.085% trifluoroacetic acid.
Ion exchange chromatography (IEX)—Proteins A, C, and D were chromatographed on an Agilent BioWAX weak anion exchange column (4.6 × 50 mm). Proteins were eluted with a gradient of NaCl in 20 mM Tris-Cl (pH 7.2). Protein B was chromatographed on an Agilent monoclonal antibody cation exchange column (4.6 × 50 mm). The protein was eluted with a gradient of NaCl in 20 mM sodium phosphate (pH 6.5).
Electrophoresis—Proteins were analyzed by capillary chip gel electrophoresis on an Experion automated electrophoresis system (Bio-Rad) under denaturing conditions in the presence of dodecyl sulfate. Analyses were carried out in the presence and absence of the reducing agent 10 mM dithiothreitol (DTT).
Size exclusion chromatography-multi-angle light scattering (SEC-MALS)—A Wyatt Treos static light scattering instrument was used to determine the masses of soluble aggregates in protein solutions after fractionation by SE-HPLC.
Results
Study I—Tungsten and Silicone Content of Prefillable Syringes
An analysis was performed to determine the amount of tungsten that could be solubilized from the barrels of prefillable syringes made of CZ and glass. Table III shows that the amount of extractable tungsten in the CZ syringes is at the level of the solvent blank, while the amount of tungsten solubilized under acidic or basic conditions from syringes made of glass is substantially above the limit of detection. The data are consistent with the fact that the CZ syringe system does not utilize a tungsten pin for insertion of the needle, in contrast to staked-needle glass syringes.
Tungsten and Silicone Content of Prefillable Syringes
An analysis was also performed to compare the silicone content of glass syringes, which use silicone oil as a lubricant, with CZ syringe barrels, which do not. The results shown in Table III confirm that in contrast to syringes made of glass, the plastic syringe barrels are silicone-free.
Study II—Long-Term Stability of Proteins Stored in Prefillable Syringes
Storage at refrigeration temperature was recommended by the manufacturers of all four biologics used in Study II. Consequently, storage at 25 °C should be regarded as an accelerated test condition.
Protein A:
The 60 kDa homodimer Protein A was stored in glass syringes and in CZ syringes for time intervals up to 1 year. SE-HPLC was used to determine recovery of soluble Protein A and to obtain evidence for the formation of soluble aggregates. Recovery of soluble protein at 5 °C and 25 °C/60% RH was quantitative from both glass and CZ syringes after 1 year. A small amount of dimer (2.5%) was present and remained nearly unchanged at 5 °C and 25 °C/60% RH in syringes made of CZ, while increasing to nearly 5% in glass syringes at 25 °C/60% RH (Table IV). There was no evidence for higher molecular weight soluble aggregates (data not shown) and sterilization of the CZ syringes by E-beam irradiation (CZE) or autoclave (CZA) had no impact on the recovery of Protein A.
Recovery of Protein A and Protein A Dimer from Stored Prefillable Syringes after 1 Year
Degradation was monitored by several techniques including RP-HPLC, IEX, and chip electrophoresis under denaturing conditions. RP-HPLC and IEX confirmed that Protein A was stable for 1 year at 5 °C in both glass and CZ syringes (Table V). However, after 1 year at 25 °C degradation of Protein A could be detected in samples from both CZ and glass syringes (Figure 1 and Table V). Chip electrophoresis under denaturing and reducing conditions indicated that only a small part of the degradation was due to fragmentation of the polypeptide into lower molecular weight species (Figure 2). Results from the three types of chromatography, SE-HPLC, RP-HPLC, and IEX, suggest that Protein A has comparable or slightly better stability when stored in syringes made of CZ than in syringes made of glass. In addition, the method of sterilization of the syringes made of CZ had no effect on the stability of Protein A. The similarity in chromatographic patterns suggests that degradation is independent of the primary packaging material.

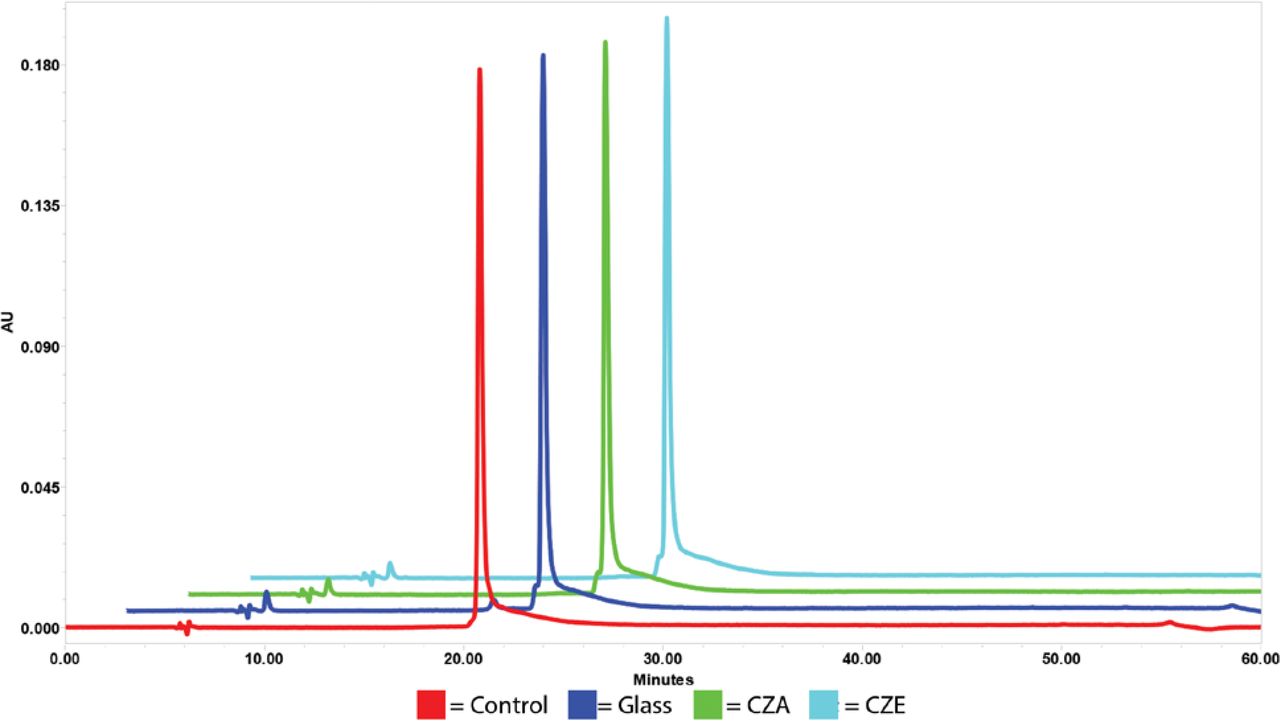
SE-HPLC of Protein A. SE-HPLC of protein A (30 μg) was performed on a Superdex S200 column. Protein was detected by absorbance at 280 nm. Data shown is the 1 year time point.

Electrophoresis of Protein A after reduction of disulfide bonds with DTT. Lane 1—Molecular weight standards; lane 2—Protein A control; lane 3—Glass 5 °C; lane 4—CZA 5 °C; lane 5—CZE 5 °C; lane 6—Glass 25 °C; lane 7—CZA 25 °C; lane 8—CZE 25 °C. Data shown is the 1 year time point. The molecular weights (×10−3) of the standards are shown on the left.
Degradation of Protein A Stored in Prefillable Syringes for 1 Year
Protein B:
The stability of the monoclonal antibody Protein B was also tested at 5 °C and 25 °C/60% RH. SE-HPLC was used to estimate the recovery of soluble protein and obtain evidence for the formation of soluble aggregates. Chromatograms of Protein B indicated that the protein was very stable after a year of storage at 5 °C and 25 °C/60% RH in both glass and CZ syringes, and recovery of soluble protein was quantitative at both temperatures (Table VI). Moreover, no high molecular aggregates were detected in samples stored at 25 °C/60% RH (data not shown).
Recovery of Protein B Stored in Prefillable Syringes for 1 Year
RP-HPLC and IEX were used to compare degradation of Protein B in glass versus CZ syringes. Analysis by RP-HPLC showed no change at 5 °C and little at 25 °C/60% RH in syringes made of glass or plastic (Figure 3). IEX confirmed that Protein B was stable at 5 °C, and although degradation could be detected at the accelerated condition (25 °C/60% RH), the amount was the same whether the protein was stored in syringes made of glass or CZ (data not shown). Chip electrophoresis in the presence of dodecyl sulfate under reducing conditions to separate the heavy and light chains of this monoclonal antibody showed no evidence for irreversible aggregation or fragmentation in either glass or CZ syringes (Figure 4). As we concluded from a similar analysis of Protein A, the stability of Protein B stored in syringes made of CZ or glass was comparable and there was no evidence that the method of sterilization of the CZ syringes affected the stability of Protein B.

RP-HPLC of Protein B. Protein B (50 μg) was analyzed by RP-HPLC on a C4 column. Protein was detected by absorbance at 280 nm. Data shown is the 1 year time point.

Electrophoresis of Protein B after reduction of disulfide bonds with DTT. Lane 1—Molecular weight standards; lane 2—Protein B control; lane 3—Glass 5 °C; lane 4—CZA 5 °C; lane 5—CZE 5 °C; lane 6—Glass 25 °C; lane 7—CZA 25 °C; lane 8—CZE 25 °C. Data shown is the 1 year time point. The molecular weights (×10−3) of the standards are shown on the left.
Protein C:
Protein C, the smallest protein of the biotherapeutics examined in this investigation, is a 16.2 kDa unglycosylated monomer. The recovery of soluble Protein C estimated by SE-HPLC from syringes held at 5 °C was about 97% whether made of glass or CZ (Table VII). Recovery decreased to approximately 90% under accelerated conditions (25 °C/60% RH) from both glass and CZ syringes, consistent with the apparent instability of this protein at higher temperatures. However, the fraction of soluble aggregates (primarily the dimer) did not increase at either temperature in syringes made of glass or plastic (Table VII).
Recovery of Protein C and Protein C Dimer Stored in Prefillable Syringes for 1 Year
To investigate potential covalent changes, Protein C was analyzed by both RP-HPLC and IEX. IEX indicated that Protein C was stable at 5 °C in both glass and CZ syringes. A small amount of degradation could be detected at 25 °C/60% RH, but it was the same in samples from both glass and CZ syringes (data not shown). However, analysis by RP-HPLC was more informative. RP-HPLC of samples stored at 5 °C were stable and comparable to the control, consistent with the results from IEX. In contrast, when samples were stored at 25 °C, a second protein species was detected that eluted 0.2 min earlier than the intact protein (Figure 5). Quantitation of the additional peak indicated that the amount of degradation was about 35% after 1 year, but nearly the same in both glass and CZ syringes. While Protein C remained stable at 5 °C in syringes made of glass or plastic, our studies showed that this protein is not stable when stored under accelerated conditions at 25 °C/60% RH in either type of syringe and irrespective of the method of sterilization of the CZ syringes.

RP-HPLC of Protein C. Protein C (27.5 μg) was analyzed by RP-HPLC on a C4 column. Protein was detected by absorbance at 280 nm. Data shown is the 1 year time point.
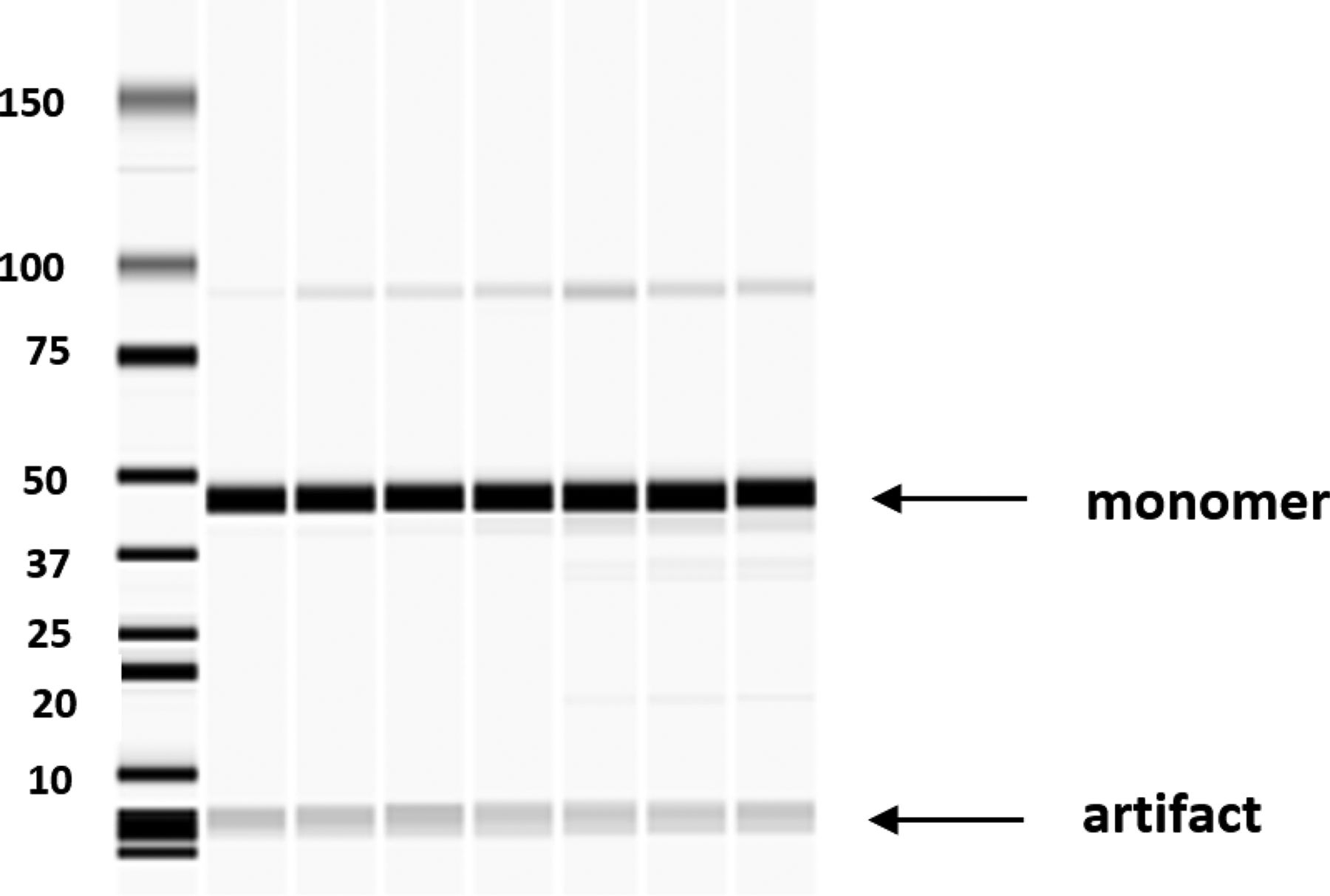
Electrophoresis of Protein C revealed one major band of approximately 16 kDa, consistent with the molecular weight of this monomeric protein (Figure 6). There is a small amount of dimer that was formed in both glass and CZ syringes at 25 °C that was not reversed by treatment with reducing agent and therefore appears to be irreversible. Several breakdown products, possibly due to contaminating proteolytic activity or a variety of nonenzymatic mechanisms (16, 17), can be seen in the 25 °C samples treated with DTT. The gel patterns appear to be the same irrespective of the whether the protein was stored in syringes made of glass or CZ sterilized by E-beam irradiation or autoclave.

Electrophoresis of Protein C after reduction of disulfide bonds with DTT. Lane 1—Molecular weight standards; lane 2—Protein C control; lane 3—Glass 5 °C; lane 4—CZA 5 °C; lane 5—CZE 5 °C; lane 6—Glass 25 °C; lane 7—CZA 25 °C; lane 8—CZE 25 °C. Data shown is the 1 year time point. The molecular weights (×10−3) of the standards are shown on the left.
Protein D:
Protein D, a 180 kDa heterodimer, is supplied in prefillable syringes made of glass that must be stored under refrigeration until administered. In this study, the protein was removed from the original glass syringes and filtered prior to loading into the glass and CZ syringes designated for this study. SE-HPLC indicated that Protein D was stable after 14 months at 5 °C in syringes made of glass or CZ. However, under accelerated conditions at 25 °C there was significant aggregation in both glass and CZ syringes, primarily in the form of dimers and trimers, as well as degradation to lower molecular weight species (Table VIII).
Protein D Recovery, Aggregation, and Degradation after Storage in Prefillable Syringes for 14 Months
SE-HPLC was also used to quantitate recovery of soluble protein. Table VIII shows that excellent recovery of the biotherapeutic was obtained from glass and CZ syringes after storage at either temperature. While there was no increase in the amount of aggregates or change in the chromatographic profile when the protein was stored at 5 °C for 14 months, after storage at 25 °C aggregation increased nearly 3-fold in both glass and plastic syringes. The amount of degradation into lower molecular weight species at 25 °C was also nearly the same in both glass and plastic syringes.
No differences from the control were detected at 5 °C or at 25 °C when Protein D was analyzed by IEX, suggesting no changes in charge (data not shown). Analysis of samples from syringes made of glass or CZ stored at 5 °C by RP-HPLC were identical to the control. Chromatograms of samples stored at 25 °C contained a new peak that eluted 4 min earlier than the parent protein and corresponding to 2% of the total, but this peak was present in samples stored in syringes made of glass or CZ (Figure 7). Chip electrophoresis of Protein D under denaturing conditions in the presence of reducing agent revealed two polypeptides, α and β, of very similar molecular weight and consistent with the heterodimeric structure of the Protein D (Figure 8). There was no evidence for the formation of aggregates or degradation of the polypeptide chains to lower molecular weight fragments in either glass or CZ syringes. Based on these analyses, there appeared to be no difference in the stability of Protein D whether stored in syringes made of glass or CZ sterilized by E-beam irradiation or autoclave.

RP-HPLC of Protein D. Protein D (50 μg) was analyzed by RP-HPLC on a C4 column. Protein was detected by absorbance at 280 nm. Data shown is the 14 month time point.

Electrophoresis of Protein D after reduction of disulfide bonds with DTT. Lane 1—Molecular weight standards; lane 2—Protein D control; lane 3—Glass 5 °C; lane 4—CZA 5 °C; lane 5—CZE 5 °C; lane 6—Glass 25 °C; lane 7—CZA 25 °C; lane 8—CZE 25 °C. Data shown is the 14 month time point. The molecular weights (×10−3) of the standards are shown on the left.
Study III—Mild Agitation
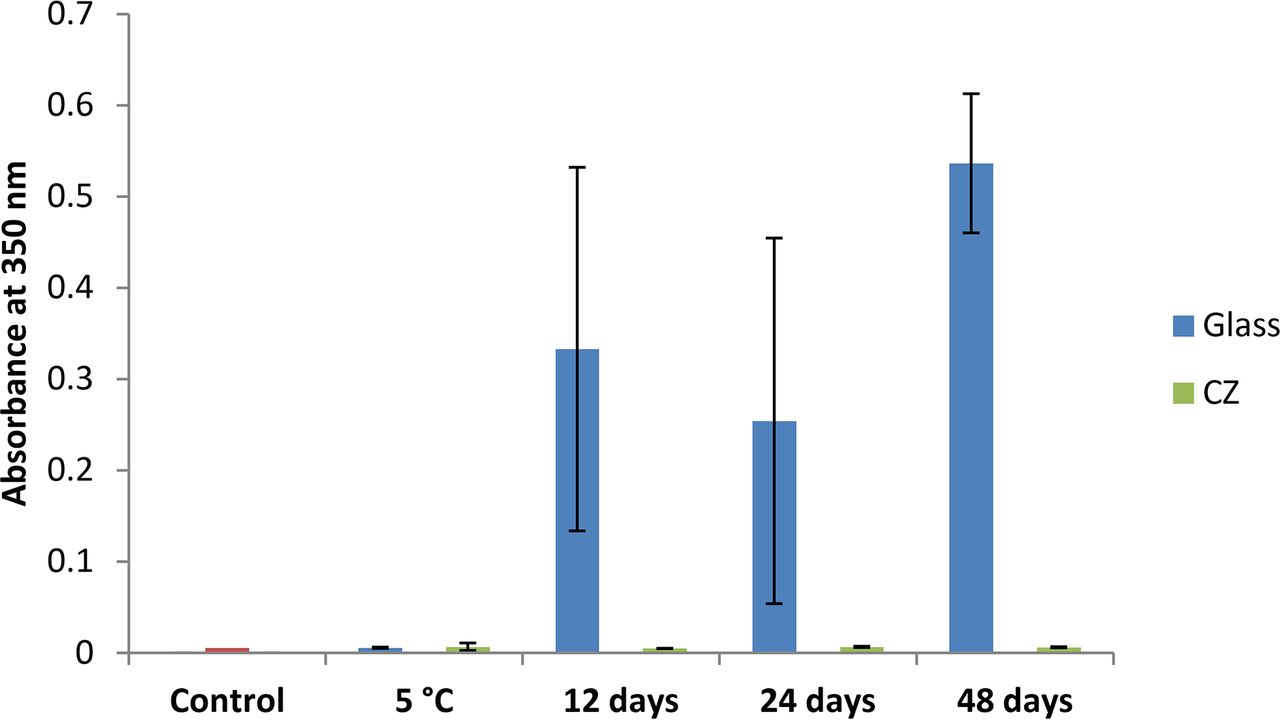
Abatacept, a 92 kDa homodimeric fusion protein with an identified silicone oil sensitivity, is administered with a silicone-free disposable syringe after reconstitution (18). A solution of the protein was agitated by end-over-end rotation in syringes made of CZ or siliconized glass, and turbidity was monitored over 48 days. Although aggregation was readily detected in siliconized glass syringes, which is consistent with a recent studies (19, 20), the aggregation of Abatacept in plastic syringes was negligible (Figure 9).

Aggregation of Abatacept during agitation. One milliliter Luer lock syringes made of siliconized glass or silicone-free CZ were filled with 1.1 mL Abatacept (2.5 mg/mL) and agitated up to 48 days. Turbidity was determined by optical density at 350 nm.
Protein E, a human IgG1 monoclonal antibody for the same therapeutic indication as Abatacept, was subjected to the same treatment. Like Abatacept, Protein E had a marked tendency to aggregate in siliconized glass syringes, but remained stable in Luer lock syringes made of CZ (Figure 10). The same result was obtained when 1 mL long syringes made of glass or plastic were compared (data not shown). Two proteins structurally similar to Protein E, human and rabbit IgG purified from pooled serum, both aggregated to a greater extent in syringes made of siliconized glass than in ones made of plastic in this stress model (data not shown).

Aggregation of Protein E during agitation. One milliliter Luer lock syringes made of siliconized glass or plastic were filled with 1.1 mL Protein E (1 mg/mL). The filled syringes were agitated up to 12 weeks. The controls remained unchanged over the course of the experiment. Turbidity was measured by spectrophotometrically by optical density at 350 nm.
The results obtained for Protein E using turbidometric methods were supported by both SE-HPLC analysis and the absorbance at 280 nm of the soluble protein recovered from the syringes (Table IX). It is clear that agitation in glass syringes results in greater loss of soluble protein than when agitated in CZ syringes. In addition to the loss of soluble protein, SE-HPLC of Protein E also indicated that agitation in glass syringes resulted in the formation of up to 5% of dimer that was not observed in chromatograms of unagitated controls or in samples analyzed from plastic syringes (Table IX). The same results were obtained whether the experiment was performed in Luer lock or 1 mL long syringes.
Recovery of Soluble Protein E and Dimer Formation in Agitated Syringes
In addition to large biotherapeutic proteins, several smaller, well-characterized proteins were subjected to agitation under the same conditions. Chymotrypsinogen A, a 25.6 kDa monomeric protein that has been used in other types of stress studies (21), was found to aggregate preferentially in syringes made of siliconized glass (Figure 11). Therapeutic insulin, a protein shown to readily aggregate in vials and tubes made of glass or plastic when subjected to high rates of agitation (22), aggregated rapidly in both siliconized glass and silicone oil–free plastic syringes under the much gentler conditions used in this investigation. However, not all proteins were sensitive to aggregation in this stress model. The industrial enzyme glucose isomerase, a 173 kDa tetrameric complex, was stable even after 84 days of agitation at RT (data not shown).

Aggregation of Chymotrypsinogen A during agitation. Chymotrypsinogen A (1 mg/mL) was agitated in Luer Lock or 1 mL long syringes (“Long-Glass”; “Long-CZ”) made of siliconized glass or silicone-free plastic for 8 weeks. Turbidity was measured at 350 nm.
To investigate whether the interaction of Chymotrypsinogen A with the hydrophobic siliconized glass surface plays a role in its aggregation, glass syringes were stripped of silicone oil using methyl isobutyl ketone. Aggregation was compared after end-over-end rotation of Chymotrypsinogen A in siliconized glass syringes with glass syringes from which the silicone had been removed as well as in syringes made of CZ. As shown in Figure 12, aggregation in siliconized glass syringes was extensive, but it was negligible in plastic syringes. In contrast, when Chymotrypsinogen A was agitated in 1 mL long glass syringes that had been stripped of silicone, the amount of aggregation was reduced nearly to control levels.

Aggregation of Chymotrypsinogen A during agitation in silicone-free glass syringes. Chymotrypsinogen A (1 mg/mL) was agitated in 1 mL long syringes made of siliconized glass, silicone-free glass, or plastic for 28 days. Glass syringes were stripped of silicone by flushing with methyl isobutyl ketone. This treatment removed greater than 95% of silicone based on quantitation of solubilized silicone using atomic absorption spectroscopy.
Discussion
The primary objective of this study was to compare the stability of several proteins stored in prefillable syringes made of siliconized glass or silicone oil–free plastic under quiescent conditions and when subjected to stress by agitation. Because the use of glass syringes has long been the standard in the biopharmaceutical industry, it was of interest to carry out a systematic comparison in performance between syringes made of glass and ones made of the cyclic olefin polymer CZ using the same set of proteins.
Study I—Tungsten and Silicone Content of Prefillable Syringes
In this study we verified that the 1 mL long glass syringes used in this investigation contained measurable amounts of both silicone oil and tungsten oxides and showed that the latter could be extracted under either acidic or basic conditions. These two substances have been shown to cause some proteins to aggregate in glass syringes, but they were found not to be present in syringes made of CZ. This result is consistent with the fact that, unlike syringes made of glass, silicone oil is not utilized for lubricity in syringe barrels made of CZ and a tungsten pin heated to high temperature is not used to form the channel for insertion of the needle.
Study II—Long-Term Stability
Study II compared the stability of four structurally diverse biotherapeutic proteins stored in syringes made of glass or CZ for a period of about 1 year at 5 °C and under thermal stress at 25 °C. The study also examined whether sterilization of CZ syringe barrels by E-beam or autoclave had an effect on protein stability. Using several analytical chromatography techniques as well as gel electrophoresis under denaturing conditions in the presence of dodecyl sulfate, we found no clear difference in stability whether the proteins were stored in syringes made of glass or CZ. All four proteins appeared to be stable at 5 °C, consistent with their recommended storage at this temperature. On the other hand, all four underwent varying levels of degradation at 25 °C, and with one exception, the amount of degradation and the chromatographic patterns were similar in samples from syringes made of glass and CZ. These results suggest that the primary container material does not have a major impact on drug stability at the higher temperature, and that stability is therefore primarily dependent on the formulation as well as on the intrinsic properties of the protein. Only the behavior of Protein A at 25 °C differed when stored in glass versus CZ syringes. For this protein we found a 90% increase over the control in the amount of dimer when the drug was stored in syringes made of glass compared to an increase of 10% after storage in syringes made of CZ. A possible explanation for the observed difference between glass and CZ is that adsorption of the monomer to the siliconized glass surface induces a conformational change that exposes hydrophobic regions of the protein. The interaction of these regions, which is entropically driven, promotes formation of the dimer, and this species is able to migrate back into the bulk solution. Whether the Protein A dimer retains biological activity is not known.
The second component of Study II addressed whether the method of sterilization of CZ syringes had an effect on protein stability. Irradiation of plastic is well known to generate free radicals, potent oxidizing agents that are highly reactive with proteins. Therefore, we compared CZ prefillable syringes that had been sterilized by autoclave with ones offered commercially that are sterilized by E-beam. Oxidative damage is an important source of protein instability, and covalent modification due to oxidation can alter a protein's physicochemical properties and lead to aggregation or fragmentation (23⇓–25). In some cases, oxidation has no effect on stability, but it may alter biological activity (26). Reaction of oxygen with proteins is generally much slower than reaction with free radicals and catalyzed oxidations, such as those involving impurities like trace metals and peroxides or exposure to light (27). However, over the expected shelf-life of many biopharmaceuticals, it is likely that various oxidative pathways can have an impact on the stability of a biologic. While most proteins contain the oxygen-sensitive amino acids methionine and cysteine, which are particularly reactive when these residues are exposed (28), photooxidation of the amino acids tryptophan, tyrosine, and histidine also occurs via pathways dependent on the presence of molecular oxygen (29). However, it is not necessary to consider this route here because the protein solutions in this study had been stored in the dark. In addition, all experiments were carried out in the presence of environmental oxygen. While definitive evidence for protein oxidation can be obtained by mass spectroscopy, we found no indirect indication, including higher levels of protein aggregation, changes in chromatographic behavior, or preferential irreversible cross-linking or fragmentation of proteins when analyzed by chip electrophoresis under denaturing conditions in the presence or absence of a reducing agent, even after a year of storage in syringes made of CZ that had been E-beam-sterilized.
Recently, Nakamura et al. have examined the degradation of the oxygen-sensitive protein erythropoietin due to oxidation in polymer-based syringes (30, 31). These investigators have also proposed that in addition to dissolved oxygen due to the high gas permeability of plastic syringes, a second cause of oxidation is related to the presence of free radicals on the syringe barrel that arise from sterilization by irradiation. The results of our study with several different proteins suggest that under our experimental conditions, there is no added risk to using polymer syringe barrels that are E-beam-sterilized over ones that are sterilized by autoclave. However, each protein should be evaluated on a case-by-case basis to identify the appropriate packaging system and method of sterilization to ensure optimal stability of the biotherapeutic.
Study III—Protein Stability under Mechanical Stress
Protein stability is a major concern with the use of prefillable syringes with biotherapeutics, particularly at high protein concentration. The undesirable formation of protein aggregates in prefillable glass syringes may be due in part to the adsorption of protein molecules onto silicone oil droplets derived from the syringe barrel. A second mechanism involves the tendency of proteins to adsorb to surfaces via hydrophobic interactions, including to the silicone oil coating on the barrel of a glass syringe or to the barrel of a silicone oil–free polymer-based syringe such as one made of CZ. These layers of adsorbed protein are believed to be a source of protein particles that can be released into the bulk solution by the movement of the air bubble during agitation (20). Other investigators have also provided evidence that the air bubble is a prerequisite for the formation of protein particles (32). When we examined the stability of several proteins under conditions of gentle agitation in the presence of an air bubble, we did not identify any that were more stable in syringes made of siliconized glass than in ones made of COP. By extracting the silicone oil coating from glass barrels, we also obtained evidence, in the case of Chymotrypsinogen A, that the silicone oil plays an essential role in the aggregation of this protein, which did not form significant aggregates in syringes made of CZ.
The results of our study suggest that the presence of a hydrophobic surface, such as the one provided by the COP plastic, even with agitation in the presence of an air bubble, is insufficient to generate protein aggregates to the same degree that was achieved in agitated syringes made of siliconized glass. While some particle generation has been shown to be attributable to bulk shear forces due to air bubble movement in the syringe (8), the role that the hydrophobic silicone oil layer plays in the initial adsorption and gelation of protein molecules cannot be duplicated by the plastic surface alone. It is noteworthy that an industrial enzyme, glucose isomerase, failed to aggregate in glass or plastic syringes under the conditions employed in these experiments. Whether this molecule's unusual stability can be attributed to poor adsorption to hydrophobic surfaces and/or to a unique structural property is not clear. Further investigation could provide some additional insight into the mechanisms of protein aggregation in prefillable syringes made from different materials.
Conclusions
The results of this study offer compelling support for the use of prefillable syringes made of CZ polymer as an alternative to syringes made of glass. CZ performed as well as glass in maintaining stability of four different proteins during storage up to a year at 5 °C and under temperature stress at 25 °C. When subjected to mechanical stress, proteins were generally more stable in silicone oil–free CZ syringes than in ones made of siliconized glass. Although sterilization of plastic is known to generate free radicals capable of reacting with proteins, no clear difference was observed in the stability of the proteins stored in CZ syringes sterilized by autoclave versus ones that had been sterilized by E-beam. The use of CZ eliminates potential issues due to exposure of sensitive biotherapeutics to silicone oil, tungsten polyanions, adhesives, and metal ions. Although each protein is unique and has to be tested to determine its stability profile, CZ and its benefits should be considered as part of this evaluation. As a plastic, CZ also has several advantages over glass including the ability to be molded into other syringe formats or cartridges for on-body injectors, and the use of CZ reduces the incidence of breakage during storage and transport as well as during administration, preventing loss of valuable product and protecting both the healthcare provider and the patient.
Conflict of Interest Declaration
The authors declare that they have no competing interests.
- © PDA, Inc. 2017
References




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Excipient and Packaging Material Impact on Glass and Polymer-Based Prefilled Syringe Functionality
- Risk Mitigation of Drug Shortages--A New Concept for Vials Designed to Improve Fill and Finish Performance
- Holistic Extractables and Leachables Program: Evaluations of Prefilled Syringe Systems for Biotechnology Products