
Abstract
Glass has long been used for packaging precious liquids, in particular pharmaceuticals. Its unique combination of hermeticity, transparency, strength, and chemical durability make it the optimal material for such an important role. Today's life-saving drugs are stored in borosilicate glasses, which evolved from applications in microscope optics and thermometers. As the glass compositions improved, so did the methods used to shape them and the tests used to characterize them. While all of these advances improved the quality of the glass container and its ability to protect the contents, problems still exist such as delamination, cracks, and glass particulates. In addition to these issues, we review new developments in glass composition development, performance, and testing in the 21st century.
Introduction: Why Is Glass an Ideal Material for Packaging Pharmaceutical Products?
Glass has been used for millennia to package various precious materials. In Egyptian times, “sacred liquids” such as fragrances, cosmetics, and oils were contained in glass vessels for preservation and transport (1). In Greek and Roman times, glass vessels served wine or displayed cremated remains and other funerary materials (2). In the 12th century, glass ampoules were used to transport anointing oils and the blood of martyrs for the Catholic Church (3). Wines have been frequently stored in glass since the 17th century when new forming equipment allowed for mass production of bottles. Glass has been used to transport and store dry and liquid pharmaceutical products since the 1700s, and now in the 21st century new drug and biologic formulations rely upon glass to provide a safe barrier from the environment (light, moisture, and contamination), enabling a long shelf life.
In each of these examples, glass is chosen to store precious liquids because it uniquely combines several properties that other materials do not. For example, glass is non-porous unlike pottery and other ceramics where inherent porosity increases the risk of evaporation losses or contamination from material trapped in pores. Glass is transparent, allowing the user to inspect the contents for degradation or contamination prior to use, and it can be colored for easy identification or added functionality such as preventing light degradation of the contents. Unlike crystalline materials, glass can be reshaped by heating into complex shapes with thin walls, and glass is gas impermeable, keeping water, oxygen, and other gases that might cause oxidation or degradation away from the liquid. The high elastic modulus of glasses prevents deformation under applied loads. Finally, glasses are more chemically durable than metals or other crystalline materials against a wide range of aqueous solution chemistries—reducing the impact of the container upon its contents.
In the 21st century, the most valuable liquids (4⇓–6) are no longer perfumes or wines but delicate pharmaceutical drug products (Table I). These delicate active ingredients increasingly require aggressive and complex excipient solutions to prevent their degradation due to changes in pH, oxidation, and other processes. Glass remains the optimal material for their storage, and it has evolved substantially over the past two centuries. Even with the advent of materials such as plastics, no new materials have been developed that are as well-suited for storing these precious materials as glass (7). Here, we review the use of glass as a primary packaging material for parenteral drugs and evolutions in its composition, forming, durability, and regulatory requirements.
Normalized Cost of a Gallon of Expensive Liquids, All Stored in Glass Containers
Glass Composition Evolution
Most glass compositions are a solution of five to ten component oxides, each serving a different function. Each component can be classified into one of five categories: glassformer, intermediate, modifier, colorant, or fining agent (8) depending upon its role within the glass structure. Instead of the periodic structures in crystals, glass is described by a series of oxide polyhedra that bond through oxygen at their corners to form a three-dimensional, continuous network. At least one glassformer oxide (SiO2, B2O3, etc.) must be present to provide viscosity and the network structure. Intermediate oxides (Al2O3, PbO, etc.) help build the network structure but are not able to form a glass on their own. Modifier oxides bring electronic charge and extra oxygen to the glass, modifying or breaking the network structure and decreasing viscosity. Modifiers include primarily alkali (Group I oxides: Li2O, Na2O, K2O, etc.) and alkaline earth oxides (Group II oxides: MgO, CaO, BaO, and others). Colorant oxides absorb light to produce color. They are typically present at low concentrations (<1 wt%) and may be intentionally added or present as an impurity with other raw materials. Colorants include most all transition metals (FeO/Fe2O3, CuO/Cu2O, CoO/Co2O3, and others), and the color produced depends upon its oxidation state. Finally, gasses released during the melting of raw materials can persist as cosmetic defects (bubbles and airlines) in final formed products, hindering visual inspection of the drug product. The fining agent is responsible for chemically aiding bubble removal during the glass melting process through the release (or uptake) of oxygen from the melt. These tend to be present at low concentrations (<0.5 wt%) and include oxides (arsenic, antimony, tin, or cerium) and halides (chlorine and fluorine).
Most glass compositions available before 1880 (including the Egyptian and Roman examples) consisted primarily of three batch materials: soda ash, limestone, and sand. These raw materials are cheap and commonly available around the world, melting easily and producing glasses known as soda-lime silicates, plate glass, or window glass (9). The term flint is sometimes used interchangeably, but refers to similar compositions that include lead oxide. Table II shows that the composition of soda-lime silicate glasses has remained relatively constant for millennia (10⇓⇓⇓–14). During the early and mid-1800s, most developments in glass packaging were around the color and shape of containers.
Analyzed Glass Compositions for Ancient and Modern Glass Containers, Showing Similar Ratios from 1500 BC to Modern Times
As early as the 1760s, glass medicine bottles were transported to the United States from western Europe, with American production of similar containers beginning in the 1850s (15). These bottles mostly stored solid and liquid preparations, as the practice of injecting medicines (subcutaneous or intravenous) did not gain in popularity until the mid- to late-1800s (16). Transparency of such containers was highly valued and, at the time, lead-containing flint glass was one of the few options that provided this desired property. More popular for its use in fine tableware, this flint glass was more expensive than standard green bottle glass (17). In 1856, Edward Perrish, a well-known pharmacist, wrote that “flint vials are considerably more expensive than the green, though they are far more elegant for prescription purposes”, with the alternative undoubtedly referring to the greenish tint of the less expensive options (15). Pharmacists in the 1700s and 1800s would charge their customers for both the container and the drug product, acknowledging the high cost of the container relative to the drug supplied within it (15).
In the 1860s, transparent glass became less expensive with William Leighton's use of a low-iron sand source to avoid the green tint usually present with traditional soda-lime silicates (17). There is, however, no specific reference to successful application of Leighton's glass for the purpose of pharmaceutical packaging. On the other hand, there appears to have been a practice in the medicine bottle industry that “decolorized” less expensive soda-lime glass by the addition of components such as manganese dioxide—with one drug company, Whitall Tatum and Co., utilizing this method through the early 1920s to produce colorless glass (18).
By contrast, some drug compounds degrade with light exposure, and clear glass is not desired for their storage (19). For example, the sensitivity of silver compounds to light was well known before 1880, so much so that the U.S. Pharmacopeia required these compounds to be stored in dark or amber-colored vials (20). Accordingly, many glass suppliers offered amber or black glass compositions for light protection—not just for drug protection but also for beer and soda packaging (9). In these glasses, iron, sulfur, or manganese were added to produce the coloration.
By 1880, advances in other fields demanded improved glass attributes and spurred composition development beyond the soda-lime silicates that had been so prevalent. Accurate temperature measurements required more precise thermometers, and advances in microscopy required optics with high refraction and low dispersion to improve magnification of small or distant objects.
In 1881, Ernst Abbe and Otto Schott partnered to systematically investigate new glass compositions, resolute to identify compositional drivers to produce these improved optical properties. Their research included more than 28 new oxides, including P, Li, Mg, Zn, Ba, Sr, As, Sb, Sn, W, and perhaps the most influential additions of Al and B oxides (21). By 1884, the partnership had developed several new compositions, one of which contained significant proportions of both aluminum and boron oxide (not significantly used prior). The addition of boron was noted to improve meltability and reduce the thermal expansion of the glass. For example, while boron-free soda-lime silicate glasses commonly expand 80–100 × 10−7/K between room temperature and 300 °C, addition of 8–12 wt% of B2O3 reduces expansion to 30–50 × 10−7/K (22). Abbe and Schott later used this glass composition to manufacture thermometer tubes (21) and gas lamp cylinder glass, which would crack in the rain and snow without the reduced thermal expansion facilitated by boron additions (23). Advances in chemistry and biology also prompted the development of low expansion, chemically durable borosilicate glasses for laboratory vessels (21, 23), although pharmaceutical storage was not the focus of their research at the time.
In 1886, a French chemist by the name of Stanislus Limousin was the first to suggest an all-glass means for storing sterile preparations; he called the container the ampoule (or ampul, ampule) (3, 24). Figure 2 shows Limousin's sketch of a glass ampoule. Shortly after, French pharmacists were the first to offer injectable medications in such containers (25). The following decades (1880–1910) saw a surge in injection-related research and manufacture, including the use of several animal and human vaccines.
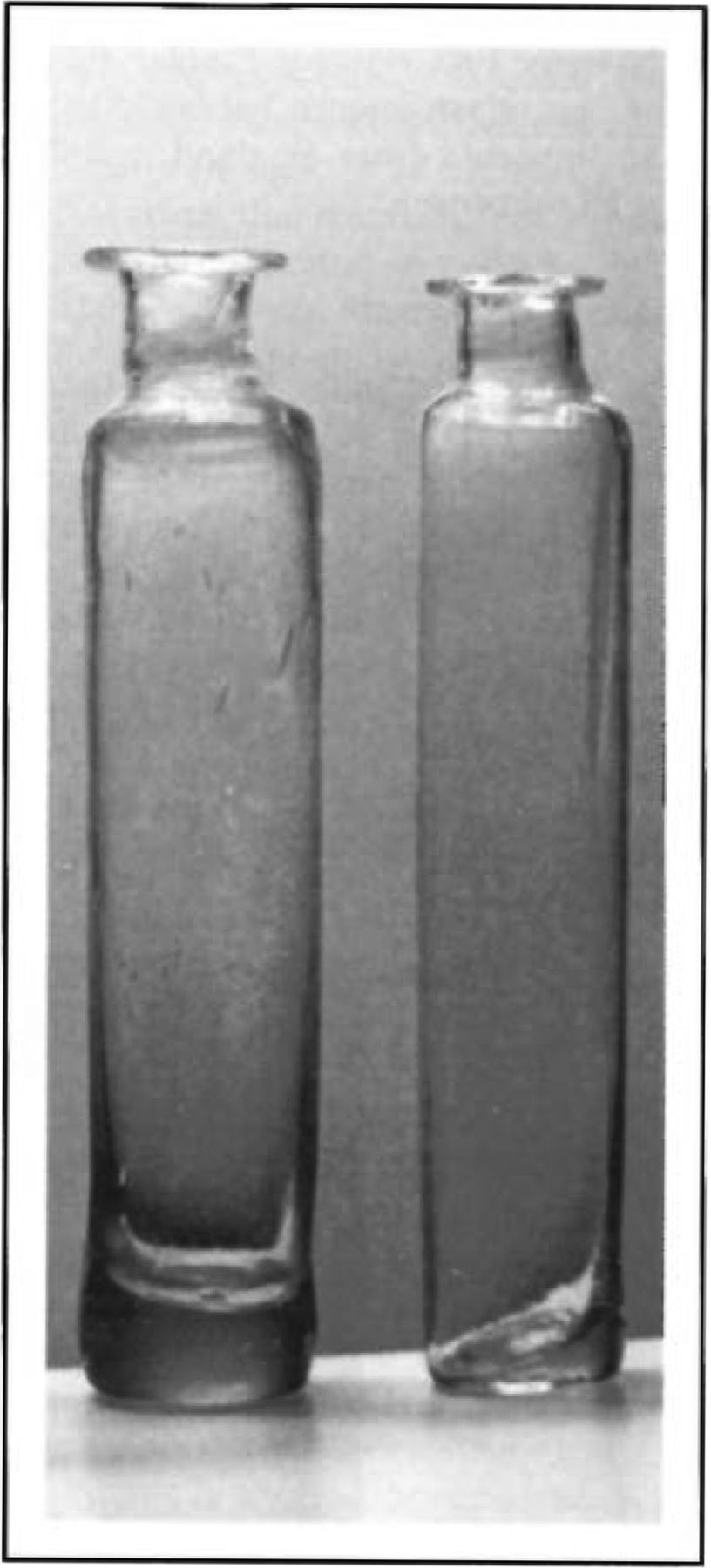
Photo of glass vials used in 1795 near Alexandria, Virginia (15).

Limousin's drawing of a glass ampoule (24).
The glass used in this initial ampoule research and manufacture was of the usual soda-lime type (25). By 1910, the borosilicate glasses intended for laboratory vessels were being used to package these parenteral solutions (26). Shortly thereafter, in 1911, Jena labs introduced a glass named alpha-glass, normal 16 III, or fiolax glass for ampoules (3, 27). Between 1912 and 1914, other glass manufacturers were pursuing modified quartz glasses (27) for pharmaceutical storage, British labs were exploring borosilicate glass compositions (28), and in 1915 Corning Glass Works introduced “Pyrex®” (code 7740) brand borosilicates for lab and consumer applications (29, 30). Due to their high fusing points, several of these glasses were not suitable for ampoule applications (25).
This flurry of glass composition development halted with the onset of World War I, especially with the Jena labs being located within Germany (31). With international trade frozen, alternate suppliers of borosilicate glasses were needed. By the 1930s, the Kimble Glass Company introduced its borosilicate glass (N51A) for lab and pharmaceutical storage applications (25). Corning introduced a similar borosilicate glass for pharmaceutical packaging (code 7800) in 1954.
With the exception of minor adjustments to remove barium, zinc, or arsenic oxides from many of the readily available borosilicate compositions (32), there were essentially no new glass compositions identified for pharmaceutical applications since ∼1930 (more than 80 years). Table III shows the composition of three borosilicate glasses measured between 1900 and 2016. As barium and zinc oxides were removed (between ∼1940 and ∼1980), the concentrations of boron, aluminum, and silicon were increased to balance. By 1990, most manufacturers of pharmaceutical glasses were struggling to support research and development of new compositions (33). Accordingly, today's pharmaceutical borosilicate glass compositions are nearly the same as they were in the 1930s.
Glass Composition for Several Commercial Borosilicates between 1900 and 2016. (A) Pyrex 33-expansion Borosilicate, (B) Schott Jena Fiolax Glass, and (C) Kimble's 51-expansion Borosilicate
Manufacturing Methods Advances
Between the late 1700s and early 1900s, glass containers for pharmaceuticals were all made via the hand-blown method, which is both time-consuming and requires skilled labor (15). More similar to art than engineering, this process produced containers of dramatically different shapes and sizes (see Figure 2). By the late 1800s, molds were increasingly used to improve the consistency of bottle shapes; and between 1880 and 1910, the bottle-forming process became fully automated, requiring minimal human intervention (41). While the manufacture of beverage bottles and food jars was quickly transitioned to the automated equipment to keep up with increasing demand, perfumery and pharmaceutical containers continued to be hand blown because smaller quantities were needed and each had a distinctive shape and size (41). By 1924, Whitall Tatum and Co. began machine-molding drug bottles (42), and the last hand-blowing operation ceased in 1942 (41).
A significant manufacturing advance in the pharmaceutical glass industry was the introduction of containers converted from glass tubing. While traditional molding processes take molten glass and form it directly into the final shape, converting operations first form molten glass into tubing and allow it to cool to room temperature. Then in a second operation, machines reheat the glass using flames while mechanical dies or tools reshape the glass into desired dimensions (vial, cartridge, syringe, ampoule, and others). The capability of reforming shapes from glass tubes was largely driven by the development of glass labware (test tubes, distillation columns, condensers, graduated cylinders, beakers, and others) while concurrently adopted for pharmaceutical applications. By 1906, the equipment necessary to convert glass tubes into these shapes was producing vials of different sizes.
Converting equipment patents evolved from semi-automated methods for forming necks in 1911 (43) to more automated methods in 1924 (44), and fully automated methods by 1960 (45). In 1965, engineering advances enabled reentrant neck geometries (to enhance glass to stopper sealing) and turret-style or vertical configuration (a shift from horizontal or linear configurations) still in use broadly today (46). Figure 3 shows examples of this evolution in container shape, size, color, and glass composition from the 1600s through today.

Evolution of pharmaceutical container shape, size, color, and glass composition from 1600s through today. From left to right: (a) manually free-blown soda-lime bottle circa 1600–1699, (b) manually mold-blown soda-lime bottle circa 1700–1799, (c) manually mold-blown soda-lime vial circa 1840–1860, (d) manually mold-blown soda-lime bottle circa 1865–1915, (e) semi-automatically mold blown soda-lime bottle circa 1880–1920, and (f) borosilicate vials: mold blown amber and tubular converted clear circa 2013–2016. Objects a–e are from the collection of the Corning Museum of Glass, Corning, NY.
Containers for parenteral packaging continue to be manufactured by both forming methods (molding and converting) today. Tubular containers are generally more desirable by pharmaceutical manufacturers for several reasons:
improved dimensional consistency (47),
decreased defects such as mold seams, wall thickness variation, etc. (48),
reduced weight through uniform wall and bottom thicknesses (48),
availability of single dose vials in smaller volumes (<3–10 mL)
lower tooling costs (48), and
enabling of more efficient heat transfer during freeze-dry processing (48).
Molded containers are desirable for some applications because
their thicker walls better resist mechanical damage (49),
they have lower extractable and leachable concentrations (47), and
they are less prone to delamination (50).
The attributes of tubular containers allow pharmaceutical manufacturers to realize improved inspection capabilities, improved container handling on automated filling machines, and greater operational efficiency and filling line yield. There are some drawbacks to the converting process (relative to molding), and these will be discussed later (see Problems Associated with Glass Packaging below).
Test Methods
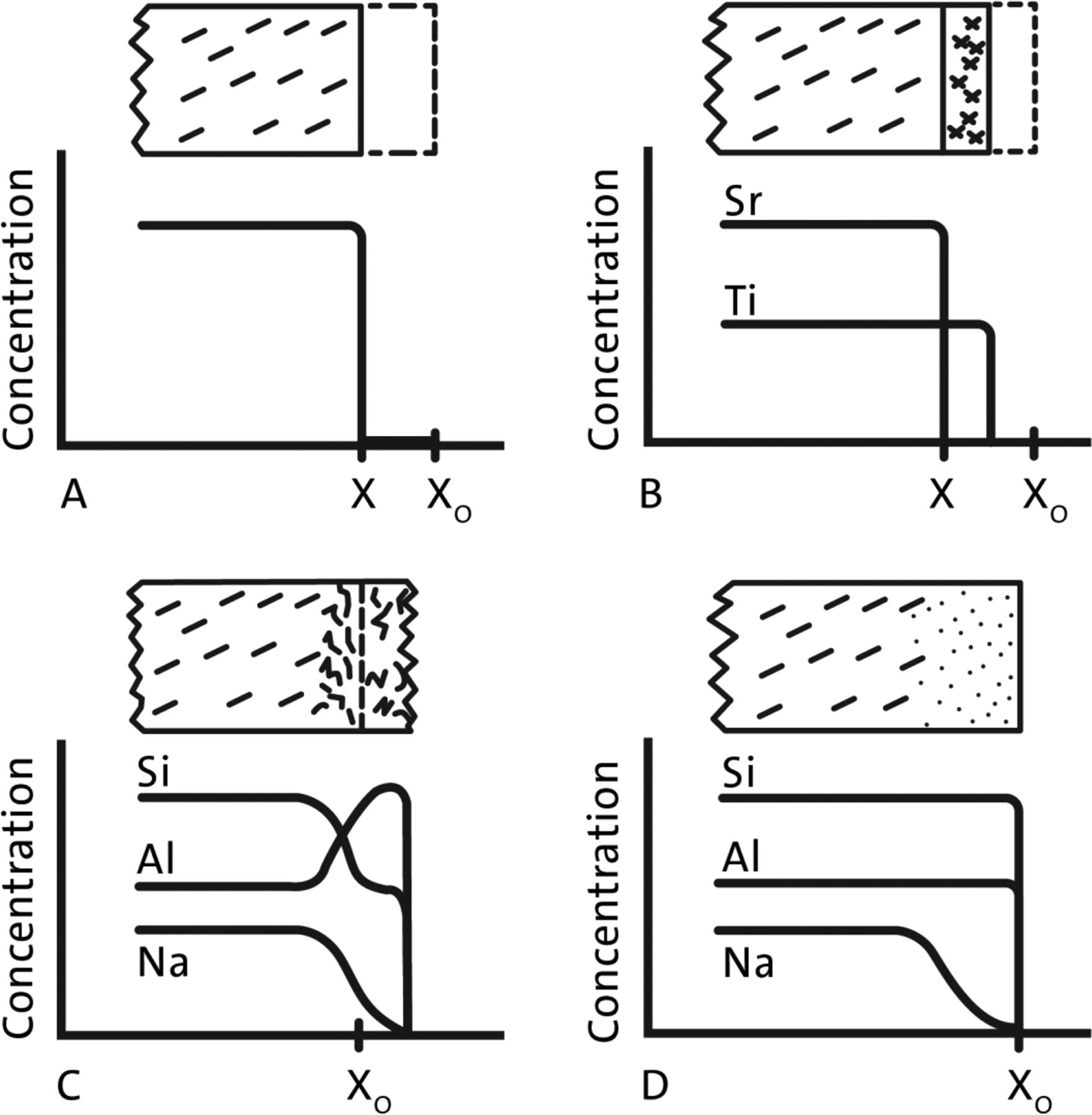
When compared to other materials (ceramics, metals, and others), silicate glasses interact less with aqueous solutions than most and are sometimes considered inert. Nevertheless, glass is not perfectly inert and does react with water, albeit at very slow rates. To complicate the characterization further, the corrosion mechanism (and associated rate) changes with solution pH. Figure 4 illustrates the impact of different corrosion mechanisms upon the glass surface, showing examples of (A) congruent dissolution, (B) incongruent dissolution, (C) reactive corrosion, and (D) selective leaching (51). Silicate glasses in acidic environments show mostly incongruent dissolution behavior, like (B), and undergo mostly congruent dissolution in basic environments as the silica portion of the network is hydrolyzed. Neutral solutions may initially show leaching (like D) and then incongruent dissolution (like B), but as the glass dissolution increases the solution pH, the mechanism will shift toward congruent dissolution (like A).
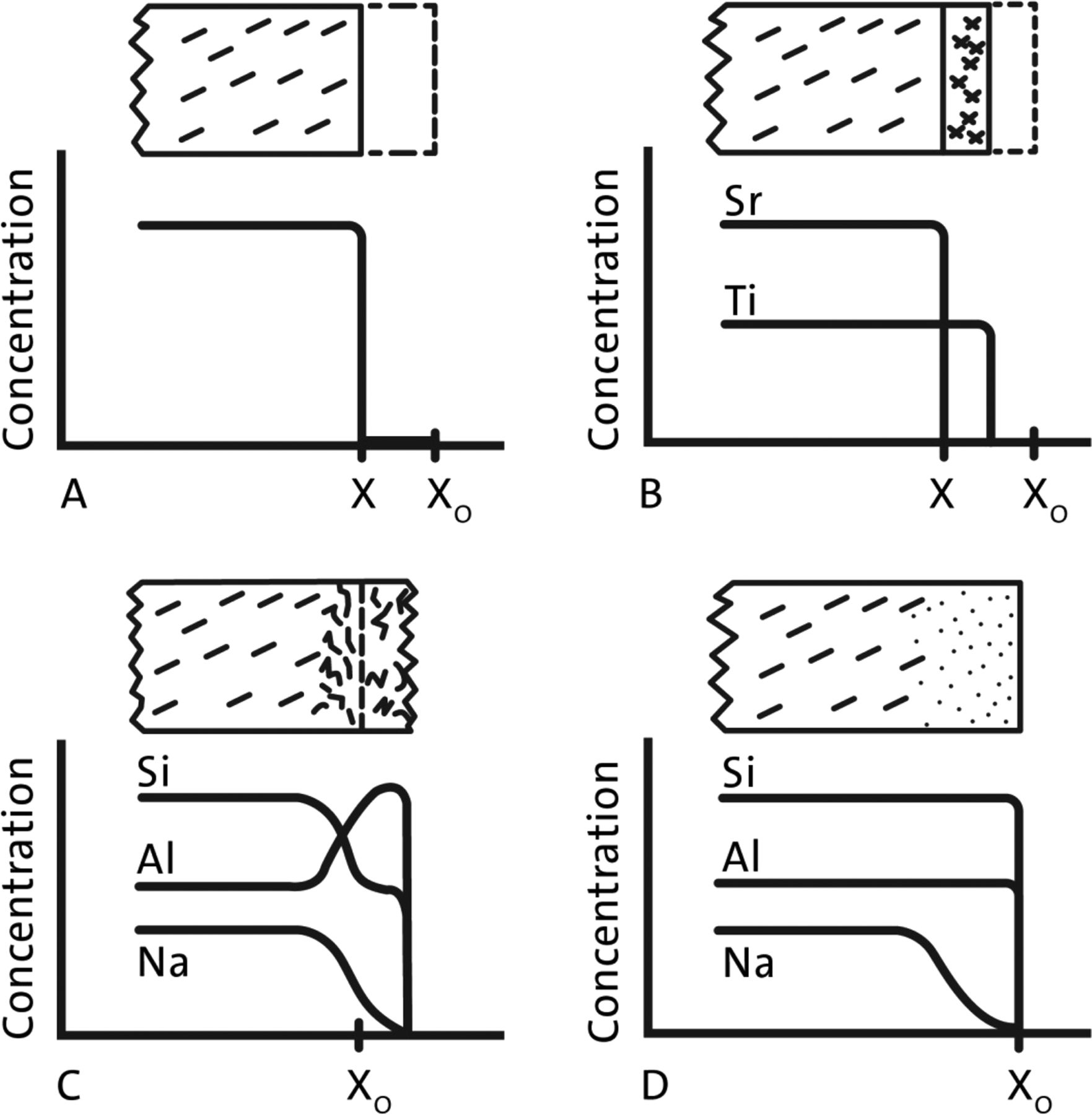
Illustration of different corrosion processes on a glass surface (51). (A) Congruent dissolution releases all elements at a single rate, (B) incongruent dissolution releasing elements at different rates, (C) corrosion of surface by chemical reaction of solvent with solid, and (D) leaching of alkali without affecting network elements.
Glass composition is the largest single influence on the chemical durability response. As such, it is important to accurately characterize the composition of the glass under analysis. In the late 1800s, glass composition determination consisted of titration of the solution produced after dissolving the glass sample in strong acids or bases. Such determination was imprecise and time-consuming, but other techniques were not yet available. Precision and speed improved dramatically with the invention of spectroscopic techniques like x-ray fluorescence, electron microprobe, or inductively coupled plasma between 1940 and 1975.
Dimbleby highlighted the importance of secondary factors upon the durability response, such as temperature of the attacking medium, length of contact period, and previous history of the glass (forming method, annealing, special treatments, and storage) (52).
Standardized test methods are needed to quantitatively compare glass compositions and secondary factors across these mechanisms, estimate extractables concentrations, or establish pharmacopeial standards. Here, chemical durability test methods are discussed in two contexts: (1) tests developed to confirm the performance of glass compositions for parenteral packaging applications, and (2) standardized tests set by compendial bodies.
Development of Different Glass Compositions
In the late 1800s, no standard methods existed for routinely assessing glass durability, and the fundamentals of the kinetic- and chemistry-dependences of glass corrosion were not yet established. While glass containers were being used to store pharmaceutical preparations (liquid, dry, and parenterals by 1900), the U.S. Pharmacopeia contained no standards regarding the identity, quality, or performance of suitable containers except that light-sensitive preparations should be stored in dark containers (20).
Abbe and Schott recognized that in laboratory applications, glass containers would experience a wide variety of solutions including alcohol, acid, base, and neutral solutions of varying temperature and concentration. In one such test, acid durability was assessed by Foerster using sulfuric acid boiling for 6 hours and expressing the result as mass loss per glass surface area (21, 53, 54), which very closely resembles modern acid tests except for the identity of the acid solution (sulfuric versus hydrochloric acids) (55). Similarly, durability in basic (high pH) solutions was assessed by Foerster using sodium carbonate solutions boiling for 3 hours and expressing the result with similar units (56). Again, this test was in use before 1900 and continues as a common standard for comparing glass durability in the 21st century (57).
The durability of a glass to attack by neutral water can be the most difficult to assess because the corrosion mechanism may change during the course of the test. Pure water interacts with glass much like a dilute acid, having little effect upon the glass network (glassformers and intermediates) while slowly extracting alkali into solution (40). Due to the low ionic strength of pure water, this release of alkali causes a shift in pH toward basic conditions. If alkali shifts the pH above about pH 9, the solution contains sufficient OH- activity to begin hydrolysis of the silicon-oxygen network. This can result in an increase in the overall corrosion rate due to the change in mechanism, from extraction of alkali to congruent dissolution of the entire glass network and all of its constituents into solution (58). Thus, any measure of the durability of a glass to attack by water is closely linked to the conditions (time, temperature, and pressure) used for accelerated testing.
During the development of borosilicate glasses in the late 1800s, neutral water or hydrolytic behavior was assessed by storing water in a container formed from the glass composition of interest, either at room temperature or under accelerated conditions (including boiling and higher temperatures). The solution produced could be analyzed either by (1) evaporating to dryness and weighing (59), (2) titrating with dilute acid (59), or (3) measuring for conductivity (60). In each case, the result was proportional to the amount of material dissolved from the glass container into solution. The acceleration conditions used in 1888 by Mylius for hydrolytic testing included boiling of glass grains in pure water for 5 hours and expressing the result in equivalents of sodium oxide (21, 61). Though the accelerating conditions are different, this is quite similar in terms of the test solution, surfaces tested, and analysis method to the current standard tests in use today (62⇓–64).
Despite pharmaceutical solutions being primarily neutral, having superior hydrolytic behavior is not sufficient to ensure suitability for use as parenteral packaging. Hovestadt noted of Mylius tests that “the densest Jena lead silicate containing 78% of lead oxide and 21% of silicic acid … [is] almost completely exempt of attack by water. … On the other hand, [these glasses] are easily decomposed by acids and alkalis” (21). Thus, proper selection of an optimal glass composition depends upon obtaining a balance of acid, base, and neutral solution durability.
Nearly a century later, in 1985, when a change in borosilicate composition was reported, suitability was justified by comparable physical properties (such as thermal expansion, viscosity, and the like) and hydrolytic performance (32). The report omits assessment of acid and base durability, which were likely affected by the change in modifier and network former content. This assumption may have negatively affected the performance of the glass material in contact with non-neutral solutions.
Standards Bodies
Pharmacopeia are standards-setting bodies responsible for developing and implementing methods to ensure the identity, strength, quality, and purity of drugs and foods, whereas formularies are typically responsible for disseminating prescribing information about drugs. The U.S. Pharmacopeia (USP) was formed and first published in 1820, while the U.S. National Formulary (NF) was first published in 1888 and eventually merged with the USP in 1975 to become one publication.
Regarding packaging for parenterals, pharmacopeia chapters should define methods for identifying and ensuring sufficient quality to package drugs described in the formulary. Between 1909 and 1915, many scientific and commercial publications compared the borosilicate and soda-lime options for ampoules (and other pharmaceutical uses), generally citing the preferred use of borosilicate (3, 26⇓–28, 65). Despite the superior performance of borosilicate glasses, the first inclusion of a glass packaging chapter would take another 10 to 15 years (in NF V, 1926) (66). That NF edition described the first method for ampules, and then the USP introduced a glass packaging chapter in 1942 (USP XII) (67) with three separate tests for distinguishing the known glass types. By the time these first standards were instituted, borosilicate and soda-lime glasses had been used in the industry for packaging injectable formulations for over 30 years.
In the 90 years since the first glass standard was written into the NF, there still are only three nominal “types” of glass performance (64). Type I containers have the highest degree of durability, due to the glass composition itself, and are suitable for most parenteral drugs. Type II containers obtain their durability due to a surface treatment that reduces the extraction of the near surface, making them suitable for most acidic and neutral parenteral and non-parenteral applications. Type III containers are the lowest degree of durability and are not generally used for parenteral powders or solutions. For a short time period before 1950, the USP described a Type IV container which was intermediate in durability between Types I & II, but how such durability was achieved is unclear.
The tests written into these standards primarily distinguish the identity of the glass type. The Glass Grains Test uses pure water and a 30 min autoclave cycle to create an extract solution that is then titrated with a dilute acid. The titrant volume limits are used to distinguish Type I containers from Types II and III. The Glass Surface Test uses pure water and a 60 min autoclave cycle to create a similar extract solution directly from the container surface, and the solution is titrated in a similar way to the grains extract solution. While the test cannot distinguish between Types I and II, it quantifies the relative performance of the surface that would be in direct contact with the drug. The Water Attack at 121 °C test and Surface Etching Test are both intended to distinguish Type II containers from Types I and III. While the Water Attack at 121 °C test conducts an extraction using pure water similar to the Glass Surface Test, the Surface Etching Test removes any surface treatments to expose the underlying bulk glass. The extract solutions from the surfaces of these are titrated, using limits (different from the Glass Surface Test) to distinguish from the other types. The Acid Attack at 121 °C test differentiates Type II and III container performance under acidic conditions from neutral and base (represented by “water attack”). A dilute acid solution is used to extract the container surface during a 60 min autoclave cycle, and the solution produced is titrated with a weak base. Finally, both the Arsenic test and the Test for containers of Type IV (only in the 12th and 13th revisions) quantify the extract levels. In one test, arsenic extracted from the glass is quantified by colorimetric titration, and in the other, the total dissolved solids are determined by evaporating the extract solution to dryness. Both tests have well-defined limits (<0.1 ppm for As, and <3.5 ppm total solids, respectively), but neither accounts for the container geometry (glass surface area to solution volume), which affects the measured concentrations.
Figure 5 is a timeline of the various USP revisions related to glass packaging, and it highlights when certain standard tests were used to distinguish glass types. It is difficult to discern from the USP texts the reasons for introduction or removal of a particular test, though one can assume that all revisions were designed to improve the resultant container quality, distinguishing capability, or measurement consistency. Perhaps the largest single revision to date occurred in 2012–2013, when Type I containers were no longer solely defined by the bulk glass grains test but additionally by the Surface Glass Test, which evaluates the hydrolytic performance of the glass surface in contact with the drug. During the same revision, the Water Attack at 121 °C test was replaced by the Surface Etching Test as the preferred method for identifying Type II glass. The new method directly tests the change in surface durability enabled by the surface treatment, and it represents a significant improvement in distinguishing capability.

Timeline of USP revisions and key milestones regarding the use of glass in parenteral packaging. The tests indicate when they were included in the USP containers chapter(s) and are grouped to illustrate the tests that distinguish each glass types.
Interestingly, the rationale for this revision (68, 69) was harmonization of test methods and limits with the European Pharmacopeia (EP) container on packaging (3.2.1). Differences between the pharmacopeia have existed for decades (25, 70), and some differences include which tests used to distinguish glass types, the specific heating and cooling portions of the autoclave cycle, the colorimetric indicator, washing procedures, and the identity of the titrant solution. Each of these differences can measurably affect the result and, ultimately, the inferred performance or identity. The upside to pharmacopeial differences and frequent revisions is that the process promotes constant improvement in methods and container selections.
Opportunities remain for improving pharmacopeial methods. Various test methods were used in the identification of the first glass compositions suitable for parenteral packaging, including a mixture of strong acid, strong base, and neutral solutions. The first pharmacopeia standards were adopted more than 30 years after borosilicate glasses were first introduced for parenteral packaging, and the selected test methods focused entirely upon performance in neutral water. Given that real drug products are often non-neutral (acidic, basic, or high ionic strength neutral) and experience higher corrosion rates than pure water, additional solutions could be included in pharmacopeial standards to assure performance and suitability under conditions more representative of real drug solutions.
All of the methods are clearly designed to establish “identity” of the glass container and infer the associated performance of that type, and, in certain cases such as the <1660> chapter, ranked performance is inferred from the relative value obtained for different containers by this method.
Many international pharmacopeia (USP, EP, Japanese Pharmacopeia, et al.) continue to improve their methods to capture the needs of the industry and improve the quality of their standards. Considering the importance of the parenteral container on patient safety and the new developments in characterization equipment and methods, materials, and drugs, the pharmacopeia continuously update their methods to reflect the most recent advances.
Problems Associated with Glass Packaging
While glass remains the preferred material for parenteral packaging containers (68, 71), it still faces challenges. Breakage (72⇓–74), cracks (75), particulates (75, 76) and delamination (50) are longstanding problems associated with existing compendial glasses, and they have resulted in numerous recent product recalls. Breakage and cracks are related to handling issues (during transport, filling, and storage), while flake production (delamination and precipitation) can be tied to the container and its interaction with the drug product.
Breakage and Cracks
Breakage is a problem for the pharmaceutical industry because it creates particulate contamination in aseptic filling areas, increases manufacturing cost and waste, and may lead to drug shortages and recalls. Glass breaks when applied loads create tensile stresses that act on existing flaws at the glass surface and cause them to propagate. Alternatively, as glass contacts materials of similar or higher hardness (including other glass containers), strength-reducing damage can be introduced that makes subsequent loading more likely to cause breakage. This damage can be introduced during glass manufacturing, pharmaceutical filling, or subsequent handling and distribution. Regardless of the mechanism, glass breakage is observed both within pharmaceutical filling lines and during customer use. For example, breakage is observed within the latest auto-injector technologies due to higher viscosity formulations (77). Some pharmaceutical manufacturers are turning to filling lines that reduce glass-to-glass contact to minimize glass damage and reduce breakage (78, 79). Other manufacturers affect breakage during customer use by treatments, such as ion-exchange (also known as chemical tempering), to strengthen the glass—like is used within the EpiPen® for injecting epinephrine to treat severe allergic reactions (80, 81). These techniques serve to preserve as much of the original glass strength as possible, or to increase the loads required to cause breakage, by installing compressive stresses that counteract the applied tensile stresses and improve the practical strength of the container.
A crack is defined as a fracture that penetrates completely through the glass (container) wall (82). Cracks can be introduced during high-temperature glass forming or by rough glass handling during filling and transportation. Cracks are problematic because they present pathways for (1) microbes and other contaminants to pass into the container's sterile contents, (2) escape of the product dosage form, and (3) allowing change of gas in the headspace content (83). In the most severe cases, contaminated doses are undetected and used, causing sepsis and death (84, 85). Current methods for addressing cracked containers include increased visual inspection during container manufacture and after filling, improved handling procedures during filling, and advancements in leak detection technologies. These methods may reduce the frequency of cracked containers leaving the manufacturing environment, but they do not address cracks introduced in the field. Despite these advances, recalls due to cracked and broken containers continue today (86).
Flakes: Low-durability Glasses, Precipitation, or Delamination
Glass flakes or lamellae refer to any thin (<1 um) but large (typically >50 um) inorganic particle produced by interaction of the drug solution with the glass (71, 87). These particles have “the potential … to cause embolic, thrombotic, and other vascular events (e.g., phlebitis); and, when administered subcutaneously, to lead to development of foreign body granuloma, local injection site reactions, and increased immunogenicity” (50). There are at least three different mechanisms for forming solid flakes of these dimensions, including leaching of low-durability glasses, precipitation, and delamination.
Low-durability Glasses:
As parenteral products were first being developed in the late 1800s, the only glasses available were soda-lime silicates with poor durability (compared to current borosilicates). These glasses were readily corroded by the drug products (including pure water) and frequently produced flakes (88). Leaching of the low-durability glass over time produces a silica-rich gel layer that, when sufficiently thick, sloughs from the underlying glass into solution. This mechanism has been frequently observed in the beverage industry, which still packages in soda-lime glasses of relatively low durability (89⇓–91).
Precipitation:
Precipitation refers to creation of a solid from components of a solution which exceed their solubility limit (3, 52, 71, 92). In parenteral solutions, this might occur by reaction of leachables of the packaging components (glass or plastic container, stopper, etc.) with the drug product (or excipient) to produce insoluble solid phases (93). For example, this can occur when barium leached from packaging components (glass, plastic, or rubber) reacts with sulfate solutions to product barium sulfate precipitates (32). Phosphate solutions are similarly prone to forming various precipitates (93, 94). Precipitates can take several shapes, including flat sheets built upon the container walls. If these sheets release from the container walls, they appear as solid flakes.
Delamination:
Delamination refers to a very specific mechanism for producing glass flakes, different from low-durability glasses and precipitation mechanisms. During the tubular converting process (and less-so the molding process), the high temperatures cause evaporation and deposition of low-melting glass constituents and formation of altered composition surface layers (87, 93, 95⇓–97). Commonly located in the heel region, these surface layers are enriched in sodium and boron species and therefore have reduced chemical durability and corrode at higher rates than the surrounding glass (98). The corrosion rate observed for these regions depends upon the degree of composition alteration during the forming process, the aqueous solution strength (pH, concentration, ionic strength, etc.), and accelerating conditions (autoclaving, pasteurization, lyophilization, storage temperature, etc.) but is substantially faster than the unaltered borosilicate glass. The corrosion rate can also be accelerated by sulfate or fluoride pre-treatments, which extract alkali from the surface of these altered layers prior to contact with the pharmaceutical solution (99). While these treatments decrease the peak concentrations of glass extractable elements present in solution, they can increase the likelihood of observing delaminated flakes because the treated surface exhibits accelerated corrosion rates.
The corrosion process occurs when water reacts with the glass surface, releasing glass constituents to solution and incorporating water into the corroded surface. This hydrated corrosion layer will swell as additional water is incorporated, creating stress between the corrosion layer and the bulk glass. Once thick enough, these corroded layers of glass are released to solution as delaminated flakes (100, 101). The appearance of flakes for containers formed with such altered surface layers can be accelerated via increased solution concentrations, temperature, sulfate treatment, pH, and also mechanical agitation (101⇓–103). Figure 6 shows an electron microscope image of the interior heel region of a borosilicate vial that contained these altered surface layers after exposure to a liquid solution. The image shows several flakes curling away from the surface in the process of release to solution, and other nearby regions where the flakes have already been released to the liquid solution.

Electron microscope image of the interior heel region of a vial which exhibited delaminated flakes after exposure to a liquid solution. The figure shows several thin flakes that have not yet released from the container surface and regions where the flakes have already been released.
While the mechanism may have first been noted in 1953 (52), the transition from molded to tubular forming processes exacerbated the frequency of delamination of borosilicate containers because of tubular forming's repeated heating and cooling processes. As tubular container manufacturing seeks higher yields and efficiency, the exaggerated heating and cooling cycles associated with increased converting speeds further increase the potential for creating these defects.
What's Next: Advances in Glass Composition, Performance, and Testing
Despite this long history of using glass to store parenteral products and other precious liquids, advances in glass composition, container performance, and testing methods suggest that further improvements may be emerging (38). Material advances are likely driven by the need to better protect the precious and costly new biopharmaceuticals products that are increasingly sensitive to aspects of the container response (pH, leachables, adsorption).
Specifically, there are reports of changes to existing borosilicate compositions to improve hydrolytic durability (38, 104, 105). There are also new compositions that have similar chemical durability without boron for preventing delamination (105⇓–107). A third category of containers places the drug in contact with glassy silicon dioxide coatings or similar materials aiming to improve breakage (108), chemical durability (109), or delamination (108⇓–110).
The existing standards describe methods for distinguishing only borosilicate, soda-lime, and sulfate-treated soda-lime glasses (64). As these new materials are adopted by pharmaceutical companies for storing their drug products, the pharmacopeia will require revision to address these alternatives. The USP has begun the revision process for the glass containers chapter (111), and perhaps this revision will include methods for characterizing new glass packaging materials.
While the glass compositions and forming methods in use today were invented 50–100 years ago, the performance needs (and expectations) of the drug product are changing. For example, newer biologic formulations are increasingly sensitive to adsorption losses. The industry as a whole (regulators, pharmaceutical companies, and container manufacturers) must address the need for improved protection of new or advanced drugs through introduction of new packaging materials.
After more than 100 years since the introduction of the borosilicate glasses for parenteral packaging, there is clearly a need for improvement and new materials are on the horizon. These new materials (and their unique attributes) have the potential to further enhance patient safety, address longstanding issues with glass containers, and empower the pharmaceutical manufacturer with options to select the optimal container material for each drug product.
Conflict of Interest Declaration
The authors declare that they have no competing interests.
Acknowledgements
The authors are thankful for the support and feedback from Katie Ruocco, Rajesh Ravikumar, and Jay Kim of Corning Incorporated. Figure 1 was reproduced with permission from Division of Medicine & Science, National Museum of American History, Smithsonian Institution. Figure 3 was reproduced with permission from Corning Museum of Glass, featuring items 54.1.10, 70.3.337, 75.4.51, 2003.4.326, 52.4.244, Collection of The Corning Museum of Glass, Corning, New York. Figure 4 was reproduced with permission from W. B. White, Theory of Corrosion in Glass and Ceramics, in Corrosion of Glass, Ceramics and Ceramic Superconductors: Principles, Testing, Characterization and Applications, by D. E. Clark and B. K. Zoitos, copyright William Andrew/Elsevier (1993). An understanding of delamination and Figure 6 was contributed by John Peanasky, Jim Hamilton, and Ron Davis at Corning Incorporated.
- © PDA, Inc. 2017
Reference
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.
- 35.
- 36.
- 37.
- 38.↵
- 39.
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- Introduction: Why Is Glass an Ideal Material for Packaging Pharmaceutical Products?
- Glass Composition Evolution
- Manufacturing Methods Advances
- Test Methods
- Problems Associated with Glass Packaging
- What's Next: Advances in Glass Composition, Performance, and Testing
- Conflict of Interest Declaration
- Acknowledgements
- Reference
- Figures & Data
- References
- Info & Metrics
Related Articles
Cited By...
- Creating an evidence-based economic model for prefilled parenteral medication delivery in the hospital setting
- Measurement of Solution Composition as an Alternative to Titration for Evaluating the Hydrolytic Resistance of Glass
- Determination of ICH-Q3D Elemental Impurity Leachables in Glass Vials by Inductively Coupled Plasma Mass Spectrometry
- Creating an evidence-based economic model for prefilled parenteral medication delivery in the hospital setting
- Investigating the Effects of the Chemical Composition on Glass Corrosion: A Case Study for Type I Vials
- An Evaluation of the Glass Vial Hydrolytic Resistance Method
- Inhibiting Sterilization-Induced Oxidation of Large Molecule Therapeutics Packaged in Plastic Parenteral Vials
- Enhancing Patient Safety through the Use of a Pharmaceutical Glass Designed To Prevent Cracked Containers